Chiari headaches are felt at the occiput – at the base of the back of the skull and upper neck. They are generally tussive in nature, where they are exacerbated by valsalva maneuvers, which generally include: coughing, sneezing, heaving, laughing hard, or bearing down (like with a bowel movement or childbirth). These maneuvers reduce cardiac output (the amount of blood coming from the heart with each heartbeat), which in turn affects the attempted flow of cerebrospinal fluid, and it increases vagal stimuli. These headaches are often accompanied with feelings of vertigo, proprioception problems, gait problems, trouble swallowing, muscle spasms (commonly starts in the eyelids – blepharospasm), memory deficits, and cognitive difficulties (usually word recollection problems).
Occipital headaches occur at the back of the lower skull (occiput) and upper neck, on one or both sides of the upper spinal cord.
Since the pushing down of the cerebellar tonsils can be congenital or acquired, we need to pay attention to other clues that our headaches might be indicating…
PRESSURE HEADACHES
Pressure headaches are generally differentiated by position.
Low-pressure headaches: pressure is generally worse when upright and relieved by laying down.
High-pressure headaches: pressure is generally worse when laying down and relieved by being upright.
EXCEPTION TO THE RULE: Internal Jugular Venous Compression Syndrome (JVCS) increases intracranial pressure, but because the jugular vein is usually more open when laying down, it is usually relieved by laying down (which often causes confusion with low-pressure symptoms).
LOW-PRESSURE HEADACHES
Those that suffer from low-pressure headaches tend to report feeling like there is an invisible pressure pushing down from the top of the head, often making it feel like your “head is going to implode.” Low-pressure headaches are characterized by being worse when upright and relieved by laying down. Low-pressure headaches are typically a sign of a cerebrospinal fluid leak (CSF Leak). The longer that the leak has existed, the less obvious the positional element – meaning the patient can be upright longer before they feel the pressure at the top of their head and they tend to need to lay down longer before getting any measure of relief. Caffeine often helps relieve low-pressure headaches.
Those that suffer from high pressure tend to feel pressure behind the eyes (often mistaken for sinus headaches) and report feeling like their “head is going to explode” from the pressure. High-pressure headaches are generally characterized by being worse when laying down – often awaking in the middle of the night or first thing in the morning with a headache, and the headache tends to dissipate to some degree after being upright for a period of time (and that period of time is different for everybody). Caffeine generally exacerbates high-pressure headaches.
All of these are most common in patients with a connective tissue disorder such as Ehlers-Danlos Syndrome.
Untreated high pressure can push the cerebellar tonsils down into the foramen magnum where it blocks the flow of cerebrospinal fluid, leading to an Acquired Chiari Malformation (usually simply diagnosed and treated as a Chiari 1 Malformation) AND the blockage of cerebrospinal fluid further increases intracranial pressure.
Untreated high pressure can cause cranial leaks – often accompanied by cerebrospinal fluid leaking through the nose (CSF Rhinorrhea) or less commonly, the ears. (This can temporarily reduce intracranial pressure and its symptoms.)
Cranial leaks (often misdiagnosed with allergies) can sometimes seal on their own as the pressure reduces, leading to rebound high pressure (which is temporary) or continued high pressure if they originally had high pressure.
Untreated spinal leaks can create a suctioning or pulling down (sag) effect where the cerebellar tonsils get lodged into the foramen magnum, creating an Acquired Chiari Malformation (usually simply diagnosed and treated as a Chiari 1 Malformation). Once there, it blocks the flow of cerebrospinal fluid and increases the pressure (which can reduce spinal pressure and increase intracranial pressure), leading to the occipital headaches and other symptoms associated with any Chiari Malformation.
Major Problem Regarding Our Diagnoses & Treatment Options:
Doctors and radiologists alike, tend to see the herniated tonsils and assume a small posterior fossa.
Most do not check for high-pressure or low-pressure, even when directly asked and symptoms are present.
When a posterior fossa decompression is finally offered, the high or low pressure is often left untreated which leads to a failed decompression.
By the time sufferers get a name to go with their symptoms, we jump at the opportunity for relief.
The “Bobble-head Sensation” – When It Feels Like Your Neck Can No Longer Hold Up Your Head
While most of us experience this feeling either intermittently or continuously, it is generally related to structural instability issues:
Craniocervical Instability (CCI, also known as Syndrome of Occipitoatlantialaxial Hypermobility) involves vertical hypermobility (back and forth sliding) of the craniocervical junction (interface between the occipital bone and the 1st and 2nd vertebrae), where the neck is no longer properly supporting the cranium. This condition can be dangerous as it often involves brain stem compression that can lead to a vast array of symptoms of Dysautonomia (dysfunction of the Autonomic Nervous System – ANS).
Subaxial Instability (SAI; also known as Cervical Instability) involves hypermobility of the C2/C3 to the C7 intervertebral discs. This condition (like most conditions involving the cervical spine) is a major cause of muscle spasms (in the neck and throughout the body at any point below the disc issues. When these neck spasms occur, they can cause the “Bobble-head sensation” where it feels like your neck can no longer hold up your head. This disc degeneration can lead to paralysis as discs compress the spinal cord.
INTRACRANIAL HYPERTENSION (IH) MEANS HIGH PRESSURE INSIDE THE SKULL.
Intracranial Pressure (ICP) is measured in millimeters of mercury (mmHg). Most scholars agree that on average, “normal pressure” should be between 5-15 mmHg, mild to moderate intracranial hypertension between 20-30 mmHg (which “requires treatment in most circumstances”), and an ICP of > 40 mmHg indicates “severe and possibly life-threatening intracranial hypertension.” [1] When high intracranial pressure is left untreated, it creates a “pushing effect” towards the only natural escape at the base of the skull (the foramen magnum), and the cerebellar tonsils in the pathway are pushed through the foramen magnum. [2]
Understanding the Monro-Kellie Doctrine (pressure-volume relationship) The association between IH/IIH and Chiari Malformation appears to be a malicious intricate pathological circle. The cranium (skull) consists of brain matter, cerebrospinal fluid, and both venous and arterial blood. A hypothesis, referred to as the Monro-Kellie Hypothesis (now better known as the Monro-Kellie Doctrine), states, “The sum of volumes of the brain, CSF, and intracranial blood is constant. An increase in one should cause a decrease in one or both of the remaining two.” Therefore, if an abundance of cerebrospinal fluid (IIH or hydrocephalus), both cranial blood volume and brain matter should be forced to deplete. This depletion is usually directed in the path of least resistance – through the foramen magnum and into the spinal canal. When the brain matter closest to the bottom of the skull (cerebellar tonsils) is pushed through the foramen magnum and into the spinal canal (an Acquired Chiari Malformation), the tonsils act like a cork and blocks the flow of cerebrospinal fluid (regardless of the size of the tonsillar descent), which in turn, continues to raise intracranial pressure.[3]
Venous Hypertension When an etiological cofactor exists (such as a space-occupying mass), it is considered Secondary Intracranial Hypertension (SIH); when no other cause was identified, it is known as Idiopathic Intracranial Hypertension (IIH) formerly known as Pseudotumor Cerebri. However, recent studies on the connection between Intracranial Hypertension and Venous Hypertension might put an end to the “idiopathic” theory.
Oxygen-rich blood travels from the heart to the rest of the body through the arterial system, then the oxygen-depleted blood returns to the heart through the venous system. We have a host of small veins in our head and they dump into a series of large veins, called sinuses.
Dural Venous Sinus Stenosis occurs when there is a narrowing of one or more of the venous sinuses (most commonly seen in the transverse sinuses or transverse/sigmoid sinus junction), which in turn compromises cerebral venous outflow through the jugular vein (stenosis/compression of the jugular vein can also result in elevated intracranial pressure [4]). Transverse Sinus Stenosis (TSS) is most common in Idiopathic Intracranial Hypertension (IIH). Depending on the study that you are reading, it is proving to be present in 90-100% of IIH patients [5]. While its connection might sound obscure if you look at it from a Monro-Kellie perspective – The blood going into the head, cannot get out at the same speed (because of the narrowed sinus). When this inflow of blood remains constant and the outflow is hindered, the transverse sinus on that side (we have two transverse sinuses, one on each side) enlarges, forcing the CSF and brain matter to reduce to maintain the volume equilibrium. This reciprocation can happen when any of the sinuses or jugular narrow (stenosis). While scholars continue to debate whether TSS is a cause or consequence of IIH, surgeons continue to decompress us without checking our pressures or decompress (the most invasive treatment) in hopes that it will lower our pressures, and patients are left with untreated high pressure still causing a “pushing down effect” and an enlarged foramen magnum for our brains to be pushed down. [2] The sagging brain once again obstructs the flow of cerebrospinal fluid by plugging the foramen magnum, and that in turn raises the intracranial pressure even more. Or, the untreated high pressure blows through the duraplasty and causes a post-operative leak, known as a pseudomeningocele.
Reducing the Risks of Post-Op IH/IIH Complications by Identifying Potential Problems Early: Brain MRIs often show indicators of Intracranial Hypertension (IH/IIH), therefore, we recommend that all Chiari patients have full brain MRIs and not just cervical MRIs.
• When the pressure builds inside of the dura mater the pressure pushes the dura and fluid inside of the crevice that holds the pituitary gland (the sella turcica or pituitary fossa). When the amount of fluid is equal to or greater than 50% and the pituitary gland size is 2mm, the condition is known as Empty Sella Syndrome. (Doctors now recognize that < 50% (where the pituitary gland size is 3-7mm) can also cause symptoms and they now refer to that as a partially empty sella.) [8]
• Slit like or flattened lateral ventricles from the increased pressure, however, when the Foramen of Monro (the aqueduct that connects the lateral ventricle to the third ventricle) is stenosed, the fluid will back-up and the lateral ventricle will not appear flattened. [7]
• Low lying or herniated tonsils (often diagnosed as a Chiari Malformation). [2]
What We Recommend BEFORE DECOMPRESSION is considered: If you have symptoms of IH/IIH accompanied by any of the MRI indicators mentioned above, it is both reasonable and prudent to ask your neurosurgeon to investigate further BEFORE DECOMPRESSION.
See a neuro-ophthalmologist to check for signs of papilledema, including Optical Coherence Tomography and Ultrasonographic B-scanning. [8]
Magnetic Resonance Venography (MRV, preferably with the ATECO technique) to check for venous stenosis of any of the cranial sinuses and/or jugular vein. Stenosis is not exclusive to the transverse sinus and it can happen in multiple sinuses simultaneously.
If overweight, consider trying to lose weight. Studies show that a weight loss of 5-10% of one’s overall body weight, when accompanied by a low-salt diet, can offer some to IH/IIH symptoms.[9]
Consider trying Diamox (Acetazolamide) and/or Topamax (Topiramate) to see if that improves the pressure headaches.
Request a lumbar puncture (spinal tap) to test your opening pressures. We recommend that it’s guided with fluoroscopy with a small gauge needle (and not the standard 22 gauge) that they allow to drip (as opposed to syringe pull) and ensure that someone is available to perform an epidural blood patch if necessary. Time should be allotted afterward to lay flat for several hours immediately following the procedure and for several days once returning home. The potential for CSF leaks is high for the EDS/Chiari patient. A doctor that marginalizes the risks ahead of time, will generally marginalize your symptoms when you are actively leaking.
ICP Bolt Monitoring can record the differences experienced in pressure over time, and how different positions affect ICP.
Note: When the intracranial pressure gets high enough, it can cause a cranial leak. This is especially true for the Ehlers-Danlos patient where the dura mater is thin and fragile. When a cranial leak decreases the intracranial pressure, the papilledema, empty sella, stenosis, and high-pressure headaches can sometimes start to revert to normal or near-normal, and the leak will affect any attempts to check intracranial pressure (reducing the pressure from what it was before the leak occurred), however, the tonsillar herniation will usually remain if the pressure gets too low. [10]
TREATMENT OPTIONS: If Venous Stenosis exists, stenting should be considered as leaving the sinus/jugular stenosed can post other health risks, and stenting is proving to have much better success with fewer complications requiring revisions. When medication fails to decrease ICP, and a stent is not an option, a Ventriculoperitoneal Shunt (VP Shunt) or Ventriculoatrial Shunt (VA Shunt) can be surgically placed to drain cerebrospinal fluid straight from the ventricle. Shunts are known for failing and often need a multitude of revisions, but even with all the revisions, it is less invasive than a decompression. Shunts under the foramen magnum should never be used as a means of controlling ICP.
For the IH/IIH patient, herniated tonsils should be assumed an Acquired Chiari Malformation (even if a small posterior fossa is evident), and by correcting the high pressure before decompression, the decompression will be less likely to fail.
Helpful Tips: If you have IH/IIH, it is best to avoid caffeine, avoid progestin based birth control, and all EDS patients should try to avoid the use of fluoroquinolones such as ciprofloxacin (Cipro), levofloxacin (Levaquin/Quixin), gatifloxacin (Tequin), moxifloxacin (Avelox), ofloxacin (Ocuflox/Floxin/Floxacin), norfloxacin (Noroxin), due to the increased risk of aneurysm.
References:
1 Rangel-Castillo, Leonardo, et al. “Management of Intracranial Hypertension.” Rangel-Castilla, Leonardo et al. “Management of intracranial hypertension.” Neurologic clinics vol. 26,2 (2008): 521-41, x. doi:10.1016/j.ncl. Feb. 2008, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2452989/>.
2 Aiken, A.H., et al. “Incidence of Cerebellar Tonsillar Ectopia in Idiopathic Intracranial Hypertension: A Mimic of the Chiari I Malformation.” American Journal of Neuroradiology; Nov. 2012, <http://www.ajnr.org/content/33/10/1901>.
3 Mokri, B. “The Monro-Kellie Hypothesis: Applications in CSF Volume Depletion.” Neurology., U.S. National Library of Medicine, 26 June 2001, <https://www.ncbi.nlm.nih.gov/pubmed/11425944>.
5 Henderson, Fraser C., et al. “Neurological and Spinal Manifestations of the Ehlers–Danlos Syndromes.” American Journal of Medical Genetics Part C: Seminars in Medical Genetics, 21 Feb. 2017, <www.onlinelibrary.wiley.com/doi/10.1002/ajmg.c.31549/full>.
7 Hingwala, Divyata R., et al. “Imaging signs in idiopathic intracranial hypertension: Are these signs seen in secondary intracranial hypertension too?.” Annals of Indian Academy of Neurology vol. 16,2: 229-33. doi:10.4103/0972-2327.112476, June 2013, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3724081/>.
8 Mollan, Susan P., et al. “A practical approach to, diagnosis, assessment and management of idiopathic intracranial hypertension.” Practical neurology vol. 14,6: 380-90. doi:10.1136/practneurol-2014-000821. May 2014, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4251443/>.
9 Thurtell, Matthew J., and Michael Wall. “Idiopathic Intracranial Hypertension (Pseudotumor Cerebri): Recognition, Treatment, and Ongoing Management.” Current Treatment Options in Neurology, U.S. National Library of Medicine, Feb. 2013, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3554852/>.
10 Pérez, Mario A., et al. “Primary spontaneous cerebrospinal fluid leaks and idiopathic intracranial hypertension.” Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society vol. 33,4: 330-7. doi:10.1097/WNO.0b013e318299c292, Dec. 2014, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4040082/>.
Some names have no meaning and some names mean absolutely everything to and about the bearer of the name. Our name falls into the latter category. Despite the more popular acronym, WTF! stands for Worth The Fight!
The origins of our name began with someone that I love to the moon and back, who was struggling with depression. This person was cutting themselves and trying to mask their pain with drugs and alcohol, and attempted suicide before I realized what was going on with them.
Life isn’t easy for a Chiari family. From the moment that I was told that my head and neck pain wasn’t just pain, but something wrong with my brain, everything in our family changed. Everything became centered on me.
“Don’t stress mom out.” “Let mom rest.” “Can’t you see how much pain she’s in?”
Surgery came just weeks after diagnosis for me. It was in hopes that I could become the wife and mother that I once was, the wife and mother that my family so desperately needed me to be. Two years after decompression, I had a revision to fix a pseudomeningocele (leak) with an SP shunt (Subgaleo-peritoneal). It was about a month after this second brain surgery that I realized that there was much more going on in my house than I’d ever dreamed.
It was just after 2 am when there was a bone-chilling pounding on our front door. It was the kind of pounding that would awaken even the heaviest of sleepers – the kind of pounding that you’d never forget. My husband and I rushed to the front room, greeted by siren lights and multiple people shining flashlights into our windows. It was a firetruck, an ambulance, and the police. We opened the door and one of the officers informed us that they had reason to believe that our daughter had attempted suicide. Words could never express the feelings that I had as I ran desperately to her room unsure about what I’d find when I opened the door. She was alive, but incoherent and unaware of her surroundings. The officer intervened to assess her condition, asking if she was able to get up and come out of her room to talk. The one officer talked to her and another two pulled us aside to talk to us, as the paramedics stood by. Everything was surreal. How could I concentrate on hearing and answering questions when I didn’t even know if our daughter was going to live or die? The officer explained that she had called a friend after taking pills with wine or champagne. The friend told his mom and together they called the police while he continued talking with her. She had initially told this friend that she was in a park across town, so the police had been scouring the park looking for an overdosed teenage girl, and when they couldn’t find her, they pinged her cell phone which led them to our home just in the nick of time. My emotions raced. How could this be when she had come to our room earlier that night, looking tired, telling us how much she loved us, and that she was going to bed? (We should have known that something was wrong, but again, I had been so lost in my own world that I couldn’t see all that my children were going through at the time.) After assessing our daughter, the attempt was deemed “credible and in immediate need of emergency care,” and she was transported by ambulance to the county hospital emergency room.
My husband and I followed in our car. At the hospital, we were informed that she had taken multiple doses of my husband’s blood pressure medications and multiple doses of my opioids. The doctors said that the first concern was her heart, “if” she survived through the night. The next concern would be liver toxicity since the opioids all contained Tylenol. And that if she survived and made it through those steps and deemed stable, she would be held on a 5150 (Involuntary Psychiatric Hold). While we prayed at her side her blood pressure dropped down to the lower 50s/20s. We called for the doctor and they told us that there was nothing more they could do (it was too late to try to pump her stomach), she would either survive the night or wouldn’t. They told us to try to keep her awake, so we walked laps around the ER every single time her blood pressure dropped in an attempt to keep her awake. I don’t know how I held up my head that night, I was running on pure adrenaline at the thought of losing my only daughter. She survived the night and while we still had to wait for the toxicity reports on the liver tests, they allowed us to walk with her over to the Psychiatric Department of the hospital.
After a twenty-four-hour evaluation, our daughter was moved to a San Francisco hospital for a week-long intensive therapy program. We couldn’t visit her for the first few days. We were limited to scheduled phone conversations. At first, she just wanted us to go get her. It’s incredibly hard as a parent to be in a position where you legally cannot just take your child home. But we knew she needed help beyond what we could offer, and eventually, she realized that she needed that too.
Over the week, she worked on herself and we worked on creating a safer environment for her to come home to (they actually have a checklist when something like this happens involving a teen). I won’t go into all the details of how we tried to safeguard our home and family after realizing that Chiari hadn’t simply set out to steal just from me physically, but its attack extended to our entire family in every way. But there was a website that I happened by that really caught my attention.
I happened upon a story “To Write Love On Her Arms” by Jamie Tworkowski. It’s a story of a group of friends learning how to fiercely love a friend struggling with depression, addiction, self-injury, and suicide. They would write the word “LOVE” on her arms; the same arms that she had been carving the words, “FUCK UP” on. They figured that if she went to cut her arms again, she’d be reminded how greatly loved she really was.
Chronic pain conditions (such as Ehlers-Danlos, Chiari Malformation, and the other comorbids) can take a toll on us and how we think, how we see our future and the value that we see us having in this world. As we see ourselves become increasingly dependent on our family members, we see the burden that it places on them, and it hurts. We know that they say that we’re ‘not a burden,’ but we see it. When we hear those that we love, deny that a burden exists, we know they’re just saying that because they love us. “It’s nothing,” they tell us. IT’S NOT NOTHING! IT’S EVERYTHING! BECAUSE THEY MEAN EVERYTHING TO US! Perhaps it would be healthier to say that ‘we’re worth the burden,’ instead. No mother can deny that having a newborn baby is a burden of love. It’s absolutely exhausting, but we know that despite the burden, no matter how hard it gets, that little baby in our weary arms is absolutely worth the work! (Just like my daughter and all that she went through, there’s nothing that I wouldn’t have given to see her through it. She was worth it!” And as I continued with my fight, I realized that I was too and if we were going to fight to win this battle, we had to have very real conversations about my fight. My family had to be allowed [encouraged even] to admit that they get exhausted without fear of hurting me or offending me. It enabled us as a family to put the blame on my conditions so that it was Chiari that has robbed us, not me. It had robbed all of us, and we weren’t going to play games and put it on anything or anyone else. We were going to fight back as a family. So if anyone has a problem with our name or our acronym, I’m perfectly okay with letting that be THEIR PROBLEM.
If you have a family member struggling with EDS/Chiari/Comorbids, whatever, you’re going to have to strengthen one another. WE HAVE TO STOP DENYING THE MAGNITUDE OF THE FIGHT, acknowledge it (every part of it), and fight back as a family, where every single person in that family KNOWS (beyond a shadow of a doubt) that they’re WORTHY! That even if we as a family must go to the ends of the earth together, it’s worth it, because each of us is WORTH THE FIGHT! And if someone forgets, write it on their arm to remind them!
This article is dedicated to my daughter, MyKaella, who taught me what it means to live knowing that we’re WTF! I’m so proud of the woman you’ve become and the woman that you helped me to become!
Making homemade stockings and cutting flowers for wreaths.
Baking treats and devouring them with hot cocoa by the tree that we spent hours decorating.
Shopping for just the right gifts and wrapping them meticulously, so those I love know just how special they are.
I remember all the traditions that we did together as a family before my symptoms hit hard.
Now, I am reduced to shopping the internet for gifts, but still, I do the best I can to find something special.
I usually start out trying to help decorate, just to end up on the couch watching everyone do what I can no longer do.
I sit here and watch despite the pain I feel from the few decorations I put on the tree because I so want to stay a part of things as much as I can, while I can, even if it’s nothing more than a shadow of what I once was.
Do they know how much I still long to be a part of it all? How much I long to be a part of them?
I sit here and as I ponder how much things have changed and all that I am now, I find myself stuck in my head.
Do they see how stuck I am?
Do they see how afraid I am, that each holiday might be the last that I have with them, and they have with me?
I’ve got to get out of my head and be present.
The best present that I can give them really is just me, fully engaged in showing them that they’re the best that has ever happened to me!
When you start to educate yourself on a condition like Chiari, your vocabulary will be challenged. Most of us study with a medical journal article opened in one tab and medical dictionary in the next. Amongst all the medical terminology you will tackle, there are probably a few terms as important to your understanding of Chiari than comorbidities and pathological/etiological cofactors. When two or more conditions tend to co-occur, they are said to be comorbid with one another. It makes no inferences of a causal relationship between the conditions, only that they co-occur. This co-occurrence deduces that a correlation exists, but when the nature of that correlation is not known, they are just said to be comorbidities. When a “causal relationship” is known or suspected, the conditions start being discussed in terms of pathology or etiology, which are similar, but not exactly the same thing.
An etiological cofactor exists when the “root cause” of a condition is known or believed to be known. That “root cause” is the etiological cofactor. When an etiological cofactor can cause a series of events or conditions that can become “direct causes” for other conditions, that series of events creates a pathology. Conditions along the path are called pathological cofactors. Understanding these cofactors is imperative in understanding Chiari and all of the comorbid conditions that accompany it.
ETIOLOGICAL COFACTOR:
Chiari Malformation often seems like a beast that wreaks havoc on our bodies on every level. Indeed it is, but as you can see from the diagram above, it really is not the “root” of everything that is going wrong. There is a bigger beast at work in so many of us, and its name is Ehlers-Danlos. It is not by chance that so many of us with Chiari have so many other conditions in common (especially conditions like Degenerative Disc Disease, arthritis and other connective tissue problems). It is not by chance that so many of us have a history of miscarriage and similar familial histories. It is not by chance that Chiari is more prevalent in females than males. And it is definitely not by chance that Chiari is running in families and they cannot find a definitive genetic link. They cannot find it because they are not looking at the beast hiding in the background.
Ehlers-Danlos Syndromes are a group of inherited disorders involving a genetic mutation in one or more of our bodies’ collagen. Collagen is the most abundant protein, making up 1/3 of the proteins in the human body, affecting our bones, skin, muscles, and connective tissue[1]. Collagen is often described as a “cellular glue” that helps hold the body together. When that glue fails to hold, everything seems to go awry; before and after birth: skulls can under-develop in utero, organs tend to prolapse, and bones begin to shift as joint laxity increases (including the bones/vertebrae at the craniocervical junction). Ehlers-Danlos is a primary “root cause” of Chiari Malformations and a majority of the other problems we have. The list in blue is far from being a complete list of conditions caused by EDS. They are commonly accompanied with Chiari because they can cause or attribute to a Chiari malformation (pathological cofactors).[2]
PATHOLOGICAL COFACTORS:
Cranial Settling occurs when the skull has dropped and the odontoid (C2/axis) enters into the foramen magnum (Basilar Invagination). This drop can further compromise the craniocervical junction and as it pushes everything down, it increases the likelihood of an Acquired Chiari Malformation.
Craniocervical Instability (CCI) & Atlantoaxial Instability (AAI) usually occurs with cranial settling and Basilar Invagination (BI). The settling and/or softening of tissue can cause a shifting of the C2 (resulting in CCI or AAI) and the cerebellar tonsils (which are already inclined to prolapse) simply drop down with each shift affecting ones ability to tilt/rotate their head.[3]
Intracranial Hypertension (IH – High Intracranial Pressure) occurs when your intracranial pressure (ICP) becomes elevated. This elevation can happen for a variety of reasons.
Space Occupying Masses (cysts, tumors or hydrocephalus) take up space inside the skull causing a “mass effect.”
When no mass effect exists, many doctors look no further and give the diagnosis of Idiopathic Intracranial Hypertension.
Because the area of the skull is fixed in an adult cranium and partially fixed in that of a child, the elements inside the fixed space (CSF, blood volume and brain matter) tend to get pushed out wherever they can (the only place that they can escape without breaking through the dura is through the foramen magnum and the brain matter that’s closest to the foramen magnum is the cerebellar tonsils).[4]
Tethered Cord Syndrome occurs when the tissue inside the epidermis adheres to the spinal cord or filum terminale. While this tethering can happen anywhere along the spinal canal, it is most common in the lower lumbar and/or sacral spine. When this adhesion happens it creates a pulling down of the spinal cord and consequently, the brainstem located at the top of the spinal cord and the cerebellar tonsils just get pulled down with it.[5]
Intracranial Hypotension (Low Intracranial Pressure, often involving a CSF Leak) usually involves a cerebrospinal fluid leak or an over-draining shunt, we will highlight the former. Ehlers-Danlos patients tend to have weak dura matter. Tears/holes in the dura can happen anywhere in the dura surrounding the brain or spinal canal and they can happen completely spontaneously (without a known cause). When the leak occurs in the spinal canal, they can create a suctioning effect where cerebrospinal fluid (CSF) is being pulled down and out, causing the intracranial pressure (ICP) to drop. The cerebellar tonsils that are already prone to prolapse (due to EDS) end up getting suctioned downward with the CSF.[6] Cranial leaks often happen when high pressure is left untreated until the high pressure causes a leak in the dura mater. In cranial leaks, fluid usually leaks through the nose or ears (less common), and you can often taste the metallic taste of the cerebrospinal fluid in the back of your throat. While both spinal leaks and cranial leaks can cause low pressure and low-pressure symptoms, and while both can start, stop, and start again spontaneously, there is an increased risk whenever there is an opening where cerebrospinal fluid leaks outside of the human body (if cerebrospinal fluid can make it out of the body, microscopic bacteria can make it inside the same opening where it can enter in the meninges).[7]
Posterior Cranial Fossa Hypoplasia (PCFH) is the only etiological cofactor listed above that is definitely congenital. The role of collagen in bone development has been long-standing, especially its known contribution to certain conditions like Osteogenesis Imperfecta. However, more recent studies are discovering the role collagen plays in congenital posterior fossa anomalies. Posterior Cranial Fossa Hypoplasia is the most commonly “acclaimed” cause of Chiari malformations, but studies show, that even when all of the other causes above are factored out, only approximately 52% of those left (that fail to meet “the diagnosis criteria” for any of the above), have a small posterior fossa.[8]
COMORBIDITIES:
While all of the conditions listed in the diagram are comorbidities, some are etiological/pathological cofactors of an Acquired Chiari (even though nearly 100% of us are told that our Chiari Malformation is congenital) and others have Chiari Malformation as their etiological/pathological cofactor:
Syringomyelia occurs when cerebrospinal fluid (CSF) is obstructed and a CSF filled cyst/cavity forms inside the spinal cord. This cyst is directly related to the obstruction of cerebrospinal fluid that can be caused by Chiari Malformation, Spinal Stenosis (a narrowing of the spinal canal, spinal cyst/tumor, a herniated disc), or irregular curvature of the spine (scoliosis). When that cyst/cavity extends into the medulla oblongata (the lowest part of the brain stem), it is called Syringobulbia, and it comes with a new set of symptoms consistent with the damage being done to the brain stem. So when Chiari Malformation exists with a syrinx, and there is no stenosis or disc problem in close proximity below it, the Chiari Malformation should be listed as the etiological cofactor for the syrinx. If more than just the Chiari Malformation is believed to be causing the syrinx, each would be more accurately described as a pathological cofactor.
Dysautonomia occurs when damage has been done to the brain stem or Vagus nerve. Whenever either of these is damaged, often from compression at/near the craniocervical junction, the autonomic nervous system can begin to dysfunction.
Confused? If you understand the causal relationships but find yourself wondering if a comorbid condition is an etiological or a pathological cofactor, think of it in terms of a domino effect. Only the first domino is the real etiological cofactor. All of the dominoes in between (on the path) are pathological cofactors. The important thing to remember in this array of medical terminology is that while everything is definitely not Chiari, it almost always shares a connection to it, and that is why so many of us have so many conditions and symptoms that doctors call unrelated! It is imperative in our fight that we know “what” we have and “why” it is happening. With such a broad spectrum of symptoms (like we all have), we must educate ourselves and not just believe the limited knowledge of our doctors.
7 Pérez, Mario A et al. “Primary Spontaneous Cerebrospinal Fluid Leaks and Idiopathic Intracranial Hypertension” Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society vol. 33,4 (2013): 330-7. doi:10.1097/WNO.0b013e318299c292, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4040082/>
TETHERED CORD SYNDROME (TCS) INVOLVES A STRETCHING OF THE SPINAL CORD, AND OFTEN YOUR MEDULLA OBLONGATA AS WELL, WHICH LEADS TO A HOST OF NEUROLOGICAL PROBLEMS.
Before we talk about Tethered Cord Syndrome, let’s first talk about the anatomy associated with the spinal column (in layman’s terms).
• The role of the vertebral column is to hold the spine strong (so it can be upright) and protect the spinal cord from injury. In a normal vertebral column, there are thirty-three vertebrae on each side (seven cervical vertebrae, twelve thoracics, five lumbar, five fused vertebrae in the sacrum and another four fused vertebrae in the coccyx).
• Each vertebra in the upper twenty-four vertebrae is separated by intravertebral discs largely composed of the fibrous protein, collagen. The main role of these discs is to allow the vertebral column to move and flex.
• The role of the spinal canal is to hold cerebrospinal fluid around the spinal cord, which not only cushions the cord against injury, but it also lubricates the cord, cleanses the cord, and brings essential nutrients that the spinal cord needs. The spinal canal is made up of several layers that form the meninges. These layers are also composed of high concentrations of collagen. The outermost layer of the meninges is the dura mater. The dura mater should be dense and strong, so cerebrospinal fluid cannot leak from it.
• The spinal cord relays messages from the brain to the nerves that allow the body to function. When part of the spinal cord is compromised, it can inhibit signals from getting to the nerves from that point downward. The brainstem (midbrain, pons, and medulla oblongata) is attached to the spinal cord at the top (the medulla and spinal cord meet at what is called the cervicomedullary junction) and the spinal cord continues down to the mid/lower back. From there it becomes a delicate elastic band of fibrous collagen-based tissue called the filum terminale that extends from the conus medullaris (the lowest point of the spinal cord before it becomes the filum terminale) to the dural sac at the S2 level.1
Chiari Malformation has many conditions that can be associated with it (comorbid conditions) and sometimes those comorbid conditions can be at the root cause (etiological cofactor) or one of the causes along the way (pathological cofactor) to the tonsils being as low as they are (making the Chiari “secondary” to one or more “other” conditions). Tethered Cord Syndrome (TCS) is one of those pathological conditions.2 Like Chiari, it is a neurological disorder; however, it is one of the spinal cord.3
Tethered Cord happens when the sticky fibrous tissue of the filum adheres to fatty/scar tissue or the dura lining of the spinal canal.1 While this tethering can happen anywhere in the spinal canal, it is most common at the lumbosacral level.4 When the tethered filum pulls the spinal cord tightly enough that it causes neurological problems, it becomes known as Tethered Cord Syndrome (TCS). Tethered Cord is most common in patients with Spina Bifida (myelomeningocele, meningocele), Spina Bifida Occulta (lipomeningomyelocele, lipomyelocele) and patients with Ehlers-Danlos Syndromes (EDS), a Hereditary Disorder of Connective Tissue (HDCT) where one or more of the types of collagen (the most abundant protein in the human body) is mutated at a cellular level. Tethered cord can be congenital or acquired. It can be obvious in childhood or symptoms may not present themselves until adulthood. Some children may develop minor signs that are overlooked by untrained medical professionals and can progress slowly or rapidly over time.
A Tethered Cord Syndrome diagnosis can be somewhat of a challenge. The signs and symptoms of the condition are not always present and when they are, they are often not recognized, so it is important to know all indicators. People with Tethered Cord (TC) can have sacral dimples, discoloration, and hairy patches on their lower back that can lead a doctor to investigate further, however, some have no external signs at all. Some have kyphosis (rounded back) and scoliosis (curved spine). Sometimes radiological criteria are not met or are ambiguous, yet an Occult Tethered Cord (characterized by the presence of symptoms with normal conus position and inconclusive findings of the filum) can still exist.5 Symptoms can be elusive as well and can happen all at once or gradually over the course of many years. Many symptoms worsen due to activity; climbing stairs has been reported as causing pain that varies from uncomfortable to excruciating.
One of the reasons that Tethered Cord is often overlooked is that many neurosurgeons are not aware of the connection it can have with a Chiari Malformation and the medical tests used for determining if a tethered cord problem exists are not always accurate or accurately read.
Magnetic Resonance Imaging (MRI)
• A lumbar MRI is usually the first step. This gives a visualization of the spinal cord in relation to the surrounding vertebrae. The actual tethering is not always obvious on MRI, sometimes the only proof of the tethering is the pulling it creates on the spinal cord. Doctors will look for the position of the conus medullaris when looking for signs that the spinal cord is being pulled. The consensus amongst most surgeons is that a normal conus should be located from the T12 to the lower L2. There is much debate on the importance of establishing evidence of a low-lying conus.5 When conus reaches the lower L2 or below, doctors should be investigating why it’s low and consider if the cord might be tethered. When looking for the location of the conus, your position can make all the difference. MRIs are generally performed supine (lying down) and the cord is not pulled as tightly as it is when upright. For this reason, upright MRIs are becoming the method of imaging preferred by most neurosurgeons looking to confirm or deny if tethering exists in a patient showing symptoms. Other signs of tethering that might be visible in a lumbar MRI include an enlarged foramen magnum, thick or fatty filum, presence of fatty tissue inside the canal, or the filum might be pulling to one side of the canal.5
• A prone MRI of the lumbar region can be an invaluable tool for those where other MRIs indicate that the filum might be pulling to one side (usually the back side) of the canal. With prone MRIs, imaging is done while the patient is lying face down (as opposed to facing up, like most supine MRIs). If the anteroposterior conus movement of >10% of the canal width was evident from the supine to the prone, then the likelihood of it pulling to one side do to tethering is less likely and more conservative management might be better appropriate than a surgical release.6
• A cervical MRI can also show signs that a tethered cord might exist. The cervical spinal cord can sometimes appear narrow from it being pulled tight. The medulla oblongata can become elongated. This happens because the brainstem is attached to the top of the spinal cord and that cord is being pulled tight, essentially pulling everything down and tight. This elongation of the medulla from the tethering can cause secondary symptoms by itself, known as Dysautonomia.
· Low/herniated cerebellar tonsils consistent with what is seen in a Chiari Malformation. When the brainstem is herniated (where part/most of the medulla is below the foramen magnum) along with the cerebellar tonsils, it is considered a Chiari 1.5 (which should be a good indicator that you might be dealing with an Acquired Chiari Malformation, where the herniated tonsils are secondary to another condition). One study quoted that out of 2,987 patients with a tonsillar herniation of 5mm or greater, 14% met the diagnostic criteria (based on “generally accepted clinical and radiographic criteria”) and 63% of the 289 patients with tonsillar herniations of < 5mm.5
· A syrinx is common with Tethered Cord, as it causes a blockage of fluid at the foramen magnum. A syrinx can develop anywhere in the spine, usually in the lower cord, but with Tethered Cord Syndrome it can develop in the lower medulla (Syringobulbia) as well because of the low brainstem is at the point of the blockage of fluid from the Chiari Malformation.
Even with an upright MRI and every symptom listed, patients are often told they do not have Tethered Cord. This is simply due to a lack of education on the subject and medical bias between doctors. It is important to make sure that you have the images viewed by a neurosurgeon that is familiar not only with Tethered Cord but Chiari and Comorbids as well. (Nearly half of the large study quoted above were referred following a failed Chiari Decompression.5) The combination of the images and the patient’s symptoms should tell the neurosurgeon if surgical intervention is required. Patients often require several consultations before they can find a knowledgeable enough physician.
What We Recommend BEFORE DECOMPRESSION is considered: If you have symptoms of TCS, especially if accompanied by any of the MRI indicators mentioned above, it is both reasonable and prudent to ask your neurosurgeon to investigate further before decompression is considered. A Tethered Cord Release Surgery prior to decompression may relieve the tension that is pulling the brainstem and cerebral tonsils downwards reducing the risk of a failed decompression. There is a chance with small tonsillar herniations that the Tethered Cord Release might allow the cerebellar tonsils to rise enough to the point that cerebrospinal fluid flow is reestablished to where decompression is no longer needed. However, failure to release a tethered cord prior to decompression surgery increases the likelihood of a failed decompression. (In fact, in the study quoted above, out of the 3,276 patients with herniated tonsils, 46% of them were referred for evaluation after a failed decompression surgery.5) An MRI of all three levels of the spine should be done to rule out other possible causes for leg/back symptoms along with urodynamic testing, an Electromyogram (EMG) Test and Nerve Conduction Study (NCS) of the lower limbs is also suggested.
TREATMENT OPTIONS:
For some, physical therapy can help with symptoms for a while. However, ultimately it will likely need to be surgically treated with a Tethered Cord Release.
Tethered Cord Release (TCR) Surgery involves the untethering of the spinal cord. An incision is made in the lumbar area, the filum terminale is separated and the factors that are tethering the spinal cord to the vertebrae are severed. Surgical treatment is not without risk and does not guarantee relief of symptoms. However, in a large study, up to 83% of adult patients report relief, 16% unchanged, and 1% report feeling worse.5 In children, the numbers are even better with 93% obtaining improved symptoms and 7% unchanged.5 Most patients describe the surgery as extremely painful for the first two weeks and “better than they ever remember feeling” (often because they have been tethered for much of their lives) after two weeks. The most common complication involves retethering (often from the scar tissue from the release) and multiple surgeries may be required over a lifetime. Finding a neurosurgeon experienced with TCRs and the surgical treatment of Ehlers-Danlos patients can sometimes help reduce the risks associated with scar tissue formation, but scar tissue can happen with even the best of neurosurgeons.
For the TCS patient, herniated tonsils really should be assumed an Acquired Chiari Malformation (even if a small posterior fossa is evident), and by correcting the tethered cord before decompression the decompression will be less likely to fail.
Special Note: There are other conditions that can present with similar symptoms. Diastasis Recti is a type of abdominal hernia common to pregnant women, those with obesity, and EDS patients. This separation in the abdominal muscles is known to sometimes cause lower back pain and many of the same pelvic floor problems seen with Tethered Cord Syndrome (TCS). Unlike TCS however, it does not usually require surgical treatment. If you suspect Diastasis Recti, we recommend that you talk to your Primary Care Physician about referring you to physical therapy to bring your abdominal muscles back together before considering Tethered Cord Release (TCR).7
[wpedon id=”4396″ align=”center”]
References:
1 Henderson, Fraser C., et al. “Neurological and Spinal Manifestations of the Ehlers–Danlos Syndromes.” American Journal of Medical Genetics Part C: Seminars in Medical Genetics, 21 Feb. 2017, <www.onlinelibrary.wiley.com/doi/10.1002/ajmg.c.31549/full>.
2 “Section of the Filum Terminale Surgery for Tethered Spinal Cord Syndrome in Patients with Chiari Malformation and Syringomyelia.” North Shore-Long Island Jewish Health System The Chiari Institute, Chiari Connection International, 02 Oct. 2006, <http://www.chiariconnectioninternational.com/docs/TCS_SFT_Explained.pdf>.
6 Aoun, Salah G., et al. “The Use of Prone Magnetic Resonance Imaging to Rule Out Tethered Cord in Patients With Structural Spine Anomalies: A Diagnostic Technical Note for Surgical Decision-making.” Cureus vol. 11,3 e4221. 11 Mar. 2019, doi:10.7759/cureus.4221. <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6510567/>.
When you start to educate yourself on a condition like Chiari, your vocabulary will be challenged. Most of us study with a medical journal article opened in one tab and medical dictionary in the next. Amongst all the medical terminology you will tackle, there are probably a few terms as important to your understanding of Chiari than comorbidities and pathological/etiological cofactors. When two or more conditions tend to co-occur, they are said to be comorbid with one another. It makes no inferences of a causal relationship between the conditions, only that they co-occur. This co-occurrence deduces that a correlation exists, but when the nature of that correlation is not known, they are just said to be comorbidities. When a “causal relationship” is known or suspected, the conditions start being discussed in terms of pathology or etiology, which are similar, but not exactly the same thing.
An etiological cofactor exists when the “root cause” of a condition is known or believed to be known. That “root cause” is the etiological cofactor. When an etiological cofactor can cause a series of events or conditions that can become “direct causes” for other conditions, that series of events creates a pathology. Conditions along the path are called pathological cofactors. Understanding these cofactors is imperative in understanding Chiari and all of the comorbid conditions that accompany it.
ETIOLOGICAL COFACTOR:
Chiari Malformation often seems like a beast that wreaks havoc on our bodies on every level. Indeed it is, but as you can see from the diagram above, it really is not the “root” of everything that is going wrong. There is a bigger beast at work in so many of us, and its name is Ehlers-Danlos. It is not by chance that so many of us with Chiari have so many other conditions in common (especially conditions like Degenerative Disc Disease, arthritis and other connective tissue problems). It is not by chance that so many of us have a history of miscarriage and similar familial histories. It is not by chance that Chiari is more prevalent in females than males. And it is definitely not by chance that Chiari is running in families and they cannot find a definitive genetic link. They cannot find it because they are not looking at the beast hiding in the background.
Ehlers-Danlos Syndromes are a group of inherited disorders involving a genetic mutation in one or more of our bodies’ collagen. Collagen is the most abundant protein, making up 1/3 of the proteins in the human body, affecting our bones, skin, muscles, and connective tissue[1]. Collagen is often described as a “cellular glue” that helps hold the body together. When that glue fails to hold, everything seems to go awry; before and after birth: skulls can under-develop in utero, organs tend to prolapse, and bones begin to shift as joint laxity increases (including the bones/vertebrae at the craniocervical junction). Ehlers-Danlos is a primary “root cause” of Chiari Malformations and a majority of the other problems we have. The list in blue is far from being a complete list of conditions caused by EDS. They are commonly accompanied with Chiari because they can cause or attribute to a Chiari malformation (pathological cofactors).[2]
PATHOLOGICAL COFACTORS:
Cranial Settling occurs when the skull has dropped and the odontoid (C2/axis) enters into the foramen magnum (Basilar Invagination). This drop can further compromise the craniocervical junction and as it pushes everything down, it increases the likelihood of an Acquired Chiari Malformation.
Craniocervical Instability (CCI) & Atlantoaxial Instability (AAI) usually occurs with cranial settling and Basilar Invagination (BI). The settling and/or softening of tissue can cause a shifting of the C2 (resulting in CCI or AAI) and the cerebellar tonsils (which are already inclined to prolapse) simply drop down with each shift affecting ones ability to tilt/rotate their head.[3]
Intracranial Hypertension (IH – High Intracranial Pressure) occurs when your intracranial pressure (ICP) becomes elevated. This elevation can happen for a variety of reasons.
Space Occupying Masses (cysts, tumors or hydrocephalus) take up space inside the skull causing a “mass effect.”
When no mass effect exists, many doctors look no further and give the diagnosis of Idiopathic Intracranial Hypertension.
Because the area of the skull is fixed in an adult cranium and partially fixed in that of a child, the elements inside the fixed space (CSF, blood volume and brain matter) tend to get pushed out wherever they can (the only place that they can escape without breaking through the dura is through the foramen magnum and the brain matter that’s closest to the foramen magnum is the cerebellar tonsils).[4]
Tethered Cord Syndrome occurs when the tissue inside the epidermis adheres to the spinal cord or filum terminale. While this tethering can happen anywhere along the spinal canal, it is most common in the lower lumbar and/or sacral spine. When this adhesion happens it creates a pulling down of the spinal cord and consequently, the brainstem located at the top of the spinal cord and the cerebellar tonsils just get pulled down with it.[5]
Intracranial Hypotension (Low Intracranial Pressure, often involving a CSF Leak) usually involves a cerebrospinal fluid leak or an over-draining shunt, we will highlight the former. Ehlers-Danlos patients tend to have weak dura matter. Tears/holes in the dura can happen anywhere in the dura surrounding the brain or spinal canal and they can happen completely spontaneously (without a known cause). When the leak occurs in the spinal canal, they can create a suctioning effect where cerebrospinal fluid (CSF) is being pulled down and out, causing the intracranial pressure (ICP) to drop. The cerebellar tonsils that are already prone to prolapse (due to EDS) end up getting suctioned downward with the CSF.[6] Cranial leaks often happen when high pressure is left untreated until the high pressure causes a leak in the dura mater. In cranial leaks, fluid usually leaks through the nose or ears (less common), and you can often taste the metallic taste of the cerebrospinal fluid in the back of your throat. While both spinal leaks and cranial leaks can cause low pressure and low-pressure symptoms, and while both can start, stop, and start again spontaneously, there is an increased risk whenever there is an opening where cerebrospinal fluid leaks outside of the human body (if cerebrospinal fluid can make it out of the body, microscopic bacteria can make it inside the same opening where it can enter in the meninges).[7]
Posterior Cranial Fossa Hypoplasia (PCFH) is the only etiological cofactor listed above that is definitely congenital. The role of collagen in bone development has been long-standing, especially its known contribution to certain conditions like Osteogenesis Imperfecta. However, more recent studies are discovering the role collagen plays in congenital posterior fossa anomalies. Posterior Cranial Fossa Hypoplasia is the most commonly “acclaimed” cause of Chiari malformations, but studies show, that even when all of the other causes above are factored out, only approximately 52% of those left (that fail to meet “the diagnosis criteria” for any of the above), have a small posterior fossa.[8]
COMORBIDITIES:
While all of the conditions listed in the diagram are comorbidities, some are etiological/pathological of an Acquired Chiari (even though nearly 100% of us are told that our Chiari Malformation is congenital) and others have Chiari Malformation as their etiological/pathological cofactor:
Syringomyelia occurs when cerebrospinal fluid (CSF) is obstructed and a CSF filled cyst/cavity forms inside the spinal cord. This cyst is directly related to the obstruction of cerebrospinal fluid that can be caused by Chiari Malformation, Spinal Stenosis (a narrowing of the spinal canal, spinal cyst/tumor, a herniated disc), or irregular curvature of the spine (scoliosis). When that cyst/cavity extends into the medulla oblongata (the lowest part of the brainstem), it is called Syringobulbia, and it comes with a new set of symptoms consistent with the damage being done to the brainstem. So when Chiari Malformation exists with a syrinx, and there is no stenosis or disc problem in close proximity below it, the Chiari Malformation should be listed as the etiological condition of the syrinx. If more than just the Chiari Malformation is believed to be causing the syrinx, each would be more accurately described as pathological.
Dysautonomia occurs when damage has been done to the brainstem or Vagus nerve. Whenever either of these is damaged, often from compression at/near the craniocervical junction, the autonomic nervous system can begin to dysfunction.
Confused? If you understand the causal relationships but find yourself wondering if a comorbid condition is an etiological or a pathological, think of it in terms of a domino effect. Only the first domino is etiological. All of the dominoes in between (on the path) are pathological. The important thing to remember in this array of medical terminology is that while everything is definitely not Chiari, it almost always shares a connection to it, and that is why so many of us have so many conditions and symptoms that doctors call unrelated! It is imperative in our fight that we know “what” we have and “why” it is happening. With such a broad spectrum of symptoms (like we all have), we must educate ourselves and not just believe the limited knowledge of our doctors.
7 Pérez, Mario A et al. “Primary Spontaneous Cerebrospinal Fluid Leaks and Idiopathic Intracranial Hypertension” Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society vol. 33,4 (2013): 330-7. doi:10.1097/WNO.0b013e318299c292, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4040082/>
When a Chiari woman passes away it changes so much for so many.
It leaves a hole in the hearts of the Chiari community because, even as dysfunctional as we are sometimes, we know we’re all in this together!
We know what it’s like to have conditions that so few understand, including our doctors.
We know how humiliating it is to watch our bodies change and our muscles deteriorate as we fight just to hold up our heads, even for just a few hours a day.
We know what it’s like to have our symptoms and pain consistently dismissed as psychosomatic.
We know what it’s like for doctors to say how easy the surgery will be only to find out that they had no clue of what they were talking about.
We know the heartbreak we feel when those we love the most choose to believe our doctors instead of us.
We know what it’s like to be told that the surgery cured us, while everything in our heads and necks seemingly rebel in disagreement.
We know what it’s like to have to fight for every aspect of our treatment, from imaging to specialist, and still have help denied to us.
We know what it’s like to have to find strength through the pain each day and still try and carry on the best that we can for those that we love so much. We long more than anything to get back to who and what we once were. To run and jump and enjoy life with those we love most, but the pain is too overwhelming. The truth is that those times that we did try left us in even more pain; so, we are forced to learn to choose what we do wisely.
We know the genetic nature of what we have, even if our doctors don’t, and we all long to figure it all out and fix this very broken medical system that relies on information that is centuries old, before our children and their children are forced to face what we face.
We know what it’s like to live in fear of leaving all those we love, as they are our reason for living.
It leaves a hole in the hearts of her family that should be respected.
To them she is so much more than a Chiari Woman, she is my wife, my mother, my daughter, my grandma, my sister, my aunt, and the love of my life.
Chiari didn’t just rob their loved one, it’s robbed the entire family for years.
They too have longed for what was and often cried behind closed doors for all that likely would never again be.
Her husband has had days where he was so petrified at the thought of losing her. Sometimes that fear manifested as anger and frustration, but it wasn’t her that he was really mad at; He was mad at the Chiari that was taking his wife from him. He regretted those words from the very minute that he gazed upon her eyes as she heard them. He couldn’t make her forget those words, they pierced her soul too deeply, so he internally committed to just try and show her why he loves her. Despite his frustrations with the situation, he admired this amazingly strong woman who was facing more pain than he could ever understand. He’s cried out to God privately for this soul mate that he committed to so many years ago. He feared losing her and he did not know how he could ever hold everything together like she did, but he had to try because there was so much was on his shoulders. He never talked much about the weight he carried in it all, because he knew what she was facing was already more than she could handle. So, he learned to grieve as silently as he could – to understand what he could, to empathize as he could, to remain as strong for her and the family as best as he could.
Her children have learned to grieve in silence as well. They learned to face life and all the obstacles they faced without making waves at home. How could they? They saw the pain that flared when things had stressed her in the past. They didn’t want to cause that again. They longed having the mom that they used to have, the mom with the strength to climb every mountain with them, the mom that made every challenge in life seem conquerable. They admired her strength and never understood how they could admire so much in her yet hate the fact that she wasn’t always there for them anymore. Even when she so desperately tried to be there the brain fog often dominated and took over the conversation entirely, this conversation that she probably wouldn’t remember for long. They resented her for it but knew that it wasn’t her fault. Like everyone else that loved her the most, they said so many things that they regretted. They knew that they often came across like they hated her, but the real truth was there was no one in the world that they longed for more. They’ve always hated seeing her in pain, yet her pain served as a constant reminder of the future that they feared in their future. They remember when she told them about the hereditary nature of the genes passed on to them, with tears in her eyes. Would they have what she had? Would they become as symptomatic? Would they have the courage to fight it as valiantly as she did? Should they have children one day? The reasons for concern were endless.
Depending on when she became symptomatic, her parents have likely spent endless days and nights in hospitals and emergency rooms. They’ve spent years learning all they could and even learned to recite her diagnoses with detailed explanations because they’d became so accustomed to these conditions that so few doctors could pronounce, much less treat. For years they made sure to always have her complete medical chart in hand with official documentation, in case they were challenged by a medical professional or anyone dared to call their daughter “a drug seeker” or “psychosomatic.” They spent countless hours trying to dull the tortuous pain they saw her go through, and spent many more hours researching creative home remedies to give her a sense of relief, even if it was only momentary. There were times they prayed for God to just go ahead and take her, so she wouldn’t be in anymore pain; and then felt guilty for even thinking it. Then one day the screaming stopped, the pain was gone, but with it so went their daughter.
As Chiarians, we all deal with thoughts of death more than “normal” people and “normal” families. We go from surgery to surgery knowing that this might be the surgery that ends our fight altogether, yet we hold on to hope that it will be the surgery that helps us to be all that we’ve yearned to be once again. Our community has found strength in our unity. As we remember those we’ve lost and face our fears about our morbidity, let us continue to unite to change this for us and our future generations that we love so much.
*This article is dedicated to all the Chiari Angels and their families, as well as those that are still fighting the fight. Hold your families close; forgive quickly and as often as necessary. We never know how much time we have and we usually never really know how much we’re truly loved until it’s too late.
**Note: This article was not to leave out all of our valiant Chiari brothers fighting the fight, it was just easier to write from one point of view.
Like any marriage, we’ve had our rocky moments. We’ve both showed our ugly sides more than we like to admit. I’m not sure when he changed, but somehow along the way in our 27 years of marriage, my husband morphed into this amazing man who is EXACTLY what I need in every way!
My husband doesn’t have the same responsibilities that most husbands have. He works full-time to provide for his family and does more than his fair share of household chores. But my husband has a wife with several chronic conditions. He has a wife that has been in some level of pain almost every day for over 18 years! He’s seen me through ten surgeries since we’ve been married, eight of them being in a five-year period. That is enough to exhaust the strongest of men, but exhausted or not he has stood by my side through all of it.
I first became symptomatic following a car accident. We were both 29 with three young kids (ages 2, 5 and 8). I was initially diagnosed with double whiplash, but when that failed to get better, I was left with no reason for why I couldn’t hold up my head. It felt like my neck lacked the strength to hold up my head for more than an hour at a time and on some days, not even that. To add insult to injury, I went without a diagnosis for over a decade. It couldn’t have been easy to stay by my side when all the doctors were saying that they couldn’t find anything wrong with me.
Over our decade without answers, I continued to decline. I started having severe cognitive decline and memory loss. I’d have periods of time where I lost my ability to walk and use fine motor skills (so I couldn’t write or pick up small things). He helped me walk to my classes and even helped me do my homework when I couldn’t write. He didn’t have the answers, but he knew that I desperately needed them, and he was determined to stay by my side even though by doing so it was putting an unfair burden on him. He didn’t have the help-meet that he needed in life. He just had this sick, scared wife, with no means to any end to her suffering.
When I was finally diagnosed, the choice for decompression was an easy one. It was 2010 and I was now 39 years old. I had lost 10 years and the possibility of getting my life back and engaging as a wife and mother again was something that I couldn’t pass up. We never expected this “easy surgery” to take the turn that it did. We knew that there was a chance that it would be unsuccessful at relieving all of my symptoms, but never in a million years did we think that decompression would open Pandora’s Box on my need for surgeries. From 2012-2015 I needed seven additional surgeries. Each surgery had its own recovery and complications. And with each additional surgery, I became increasingly dependent on my husband for help, but not once did he complain. This was affecting his life too, but not once did he concentrate on that. Not once did he think of it as being unfair to him to have to care for me, even though it really was. I’m now covered with scars on my left side from my neck to my groin, one night he raised my pajama shirt and gazed intensely upon them. He started kissing them. When he got to the scars covering my stomach, I pushed him away and with tears in my eyes, I told him that I wasn’t comfortable with him touching me there. He looked me in the eyes and told me that he didn’t see me the way that I see myself. He said that when he sees my scars, he’s reminded of all that I’ve had to fight through and what a strong woman he’s married to. “I wish that you could see yourself the way that I see you,” he exclaimed. All my insecurities just melted with his words of affirmation.
This man who vowed to love me for better or worse, richer or poorer, in sickness or in health, really meant it, and those vows were continually put to the test every day of his life. And he wasn’t seeing the polished-up version of me that others tend to see. He saw the frustrated me, the defeated me, the hopeless me. The me that went from one pair of pajamas to another. The me that gained over a hundred pounds on nerve meds that ultimately made me worse. The me that started to stutter and slur and hated myself for it. The me that drooled in front of people and whose nose ran uncontrollably when I sat down to eat. The me that lost control of both her bladder and bowels and that had to wear a diaper for years. The me that no longer could wipe herself or shower without his help. The me that took so much of my pain and frustrations out on him, when he’d take all of it upon himself in an instant if he could save me from it. Not only does he not complain or criticize, but he became my biggest cheerleader in life!
He listened to me as I read studies to increase my knowledge on what I’m facing. He lets me yell to him about the incompetency of doctors. He’d make small jokes to help me make light of the seriousness at hand. When he forgot things, he’d say that he was having a “Chiari moment.” I’d remind him that he wasn’t the one with Chiari and he insisted that it was sympathy pains. When he developed a herniated cervical disc and we looked at his MRIs together, the first words that came out of his mouth were, “well, I don’t have a Chiari Malformation,” as he pointed at the cerebellar tonsils. I often feel so unworthy of his love, yet if you talked to him, he’d tell you how unworthy he is of my love.
There’s no denying his real role in my life; he’s my hero!
*This article is dedicated to my husband, Johnny (my hero and the love of my life) and to all the other couples trying to hold a marriage together through this crazy fight we face.
Palliative Care: An Essential for EDS & Chiari Families
When I was first diagnosed with Chiari Malformation, I believed everything that my neurosurgeon told me. I was originally diagnosed with a Chiari 1 Malformation. I was told that it was congenital and due to my mother either using drugs or not getting proper prenatal care, which was crushing to hear, but not all that unlikely since I was born in the early 1970s. Little did I know, that these assumptions weren’t based on my findings, but on what textbooks have said since before the advent of the MRI in the early 1980s. Sadly, the percentage of Chiari patients that are given these same faulty assumptions remains near 100%. It didn’t take much time after my decompression surgery for me to realize, that it wasn’t quite as easy or cut-and-dry as it had been made out to be. When you have a connective tissue disorder, that is the root cause behind your Chiari diagnosis, the risk of postoperative complications is high, especially when pathological conditions went undiagnosed and untreated when the decompression was done. The difficulties of having a genetic mutation that can cause problems throughout your entire body, can make a patient seem like a hypochondriac, and that is exactly what most doctors think when they have a subpar understanding of Ehlers-Danlos Syndromes. When something goes wrong structurally, it can cause a cascading effect that manifests throughout the body. We go into the Chiari fight understanding that something is wrong with our brain and neck, but when it crosses over to problems with the autonomic nervous system (for instance), we don’t realize that the continued compression on our brainstem is why our hearts are now beating so fast, why we are now so short of breath, or why we are having fainting spells. We find ourselves wishing for someone, or a panel of experts to help us navigate through it all. While it is still far from the panel that we really need, Palliative Care can offer help with some essentials.
What is Palliative Care?
Palliative Care (pronounced “pal-lee-uh-tiv” care) is a subspecialty of medical care, where an interdisciplinary team of professionals (both medical and social) are committed to helping provide “relief from symptoms and stress” for patients with serious, life-altering illnesses, and their families. [1] Palliative Care is “supportive care,” by professionals committed to you as a patient with a serious illness! Your Palliative Care Team generally consists of a Palliative Doctor, a nurse, pharmacist, social worker, nutritionist, and a chaplain [2] (all as needed). Together, they will seek to:
Ease symptoms and/or help control pain to relieve suffering
Help improve your quality of life
Help coordinate with your care team
Assist with stress, fears, anxiety, and/or depression in the patient, caregiver, and/or family
Help you create a plan for end-of-life care (directives)
Benefits to Palliative Care:
Both Chiari Malformations and Ehlers-Danlos Syndromes are relatively complex. Both conditions can spur a vast array of symptoms. One of the objectives of your Palliative Team is to help you find a way to alleviate symptoms and/or help you with coping mechanisms through them.
Because Palliative Care is designed for patients with “serious” medical conditions, being accepted as Palliative Care patient, means that they recognize the seriousness of our condition. For those of us that have spent years/decades with our symptoms being dismissed, this alone is no small thing.
The CDC Guideline for Prescribing Opioids, as well as many of the state laws regarding the same, have exemptions for palliative patients (along with cancer and end-of-life patients). Doctors can still decide to discontinue prescriptions, taper your prescriptions, or require an “opioid contract,” but it will be 100% by their choice, and not due to CDC Guidelines and laws. Although, you may have to tell them that. [4]
Misconceptions Surrounding Palliative Care:
While it is outlined in the U.S. Department of Heath & Human Services (NIH) under the “National Institute on Aging” (NIA), there is NO AGE CRITERIA to qualify as a Palliative Care patient. [1]
While Palliative Care is frequently listed beside Hospice Care and/or End-of-Life Care, there is no national requirement for a patient to be in an end-of-life situation (or even an expected early demise). [1] Hospice care falls under palliative care, but palliative care expands beyond the scope of just hospice. Palliative care may begin at any stage of a serious illness. [2]
You can continue treatments (even curative treatments) with your personal doctor/specialist, while receiving palliative care. There is no “incurable condition” requirement for a serious condition under palliative care. [2][3] In fact, a patient can qualify and receive Palliative Care whether their illness is curable, chronic or life-threatening. [2]
You do not need to wait until your condition reaches a certain level of severity, you can start with Palliative Care at any stage of your illness. In fact, Palliative Care works best when it begins as early as possible in the illness, as some symptoms may be avoidable or more manageable if addressed early.
Palliative Care does not replace or override your pain management doctor, or any of our doctors for that matter. Instead, we give them permission to discuss our case with our medical professionals, so they can help coordinate our care, especially in regard to our pain/suffering and quality of life care.
Your Palliative Care Team will not consist of the medical specialists that we specifically need, but they can help navigate you to the type of doctor you may need and discuss these recommendations with your doctors.
Problems Surrounding Palliative Care:
Primary Care Doctors (who are supposed to be offering referrals to Palliative Care for their patients with serious medical conditions) often fail to fully understand the spectrum of Palliative Care. Because of their faulty understanding, most of us are never offered Palliative Care, and when we request it, we are often told that it is equivalent to hospice care or set aside for hospice patients, and therefore they believe that we do not qualify. THEY ARE WRONG!
Our medical professionals often fail to recognize just how “serious” of a condition and life-altering Chiari and EDS really are (on us as patients and on our families).
Not all insurance companies cover Palliative Care. Because some insurance companies fail to see the seriousness of our conditions, qualifying may be difficult. Private insurance and HMOs are more likely to offer Palliative Care. Different states have different policies regarding the level of Palliative Care (if any) they offer. [2] If cost concerns are an issue, the social worker on your Palliative Team can assist you in ways that might help you qualify. [3]
[wpedon id=”4396″ align=”center”]
References:
1. “What Are Palliative Care and Hospice Care?” U.S. Department of Health and Human Services, National Institute on Aging, 17 May, 2017. <https://www.nia.nih.gov/health/what-are-palliative-care-and-hospice-care>
2. “Frequently Asked Questions About Hospice and Palliative Care.” American Academy of Hospice and Palliative Medicine. <http://palliativedoctors.org/faq>
3. “Handout for Patients and Families.” Center to Advance Palliative Care. <https://getpalliativecare.org/handouts-for-patients-and-families/>
4. “CDC Guideline for Prescribing Opioids for Chronic Pain.” Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Unintentional Injury Prevention. 29 Aug, 2017 <https://www.cdc.gov/drugoverdose/prescribing/guideline.html>
Disclaimer: The information provided on our website is strictly for educational purposes in order to help further the understanding of Chiari and its associated conditions. You should in no way use this site as a replacement for diagnosis, treatment, or medical advice from a qualified medical professional.



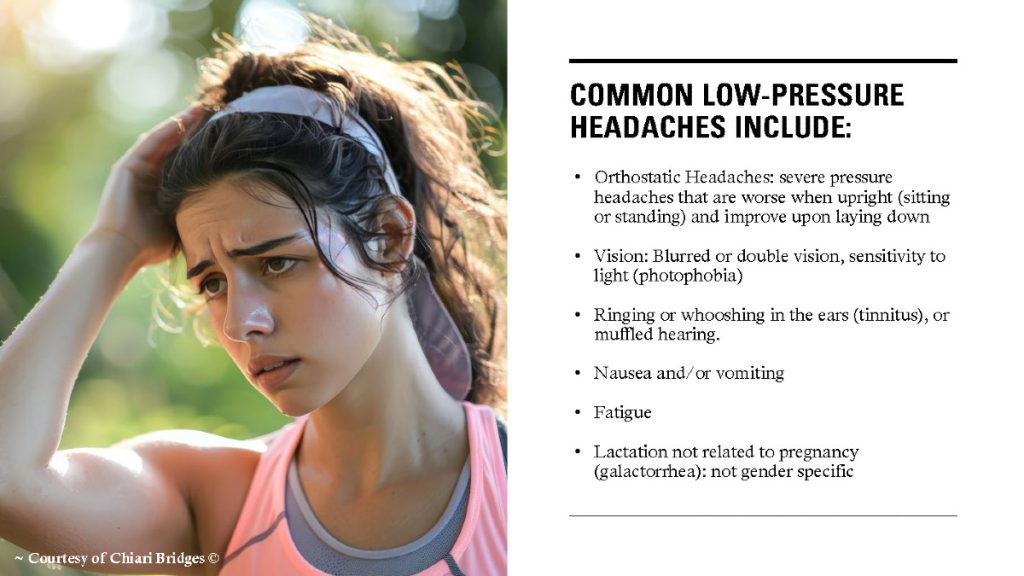
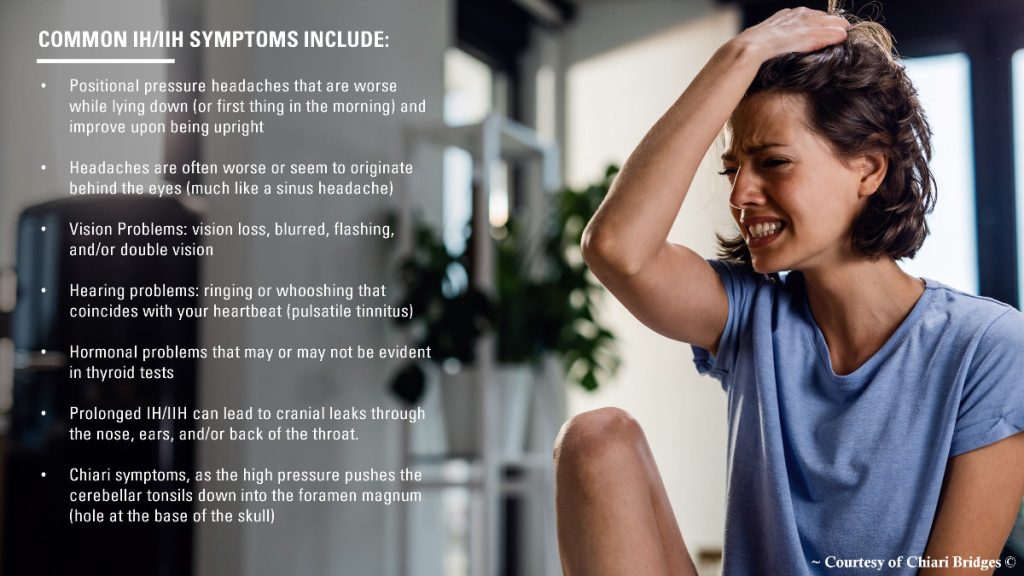
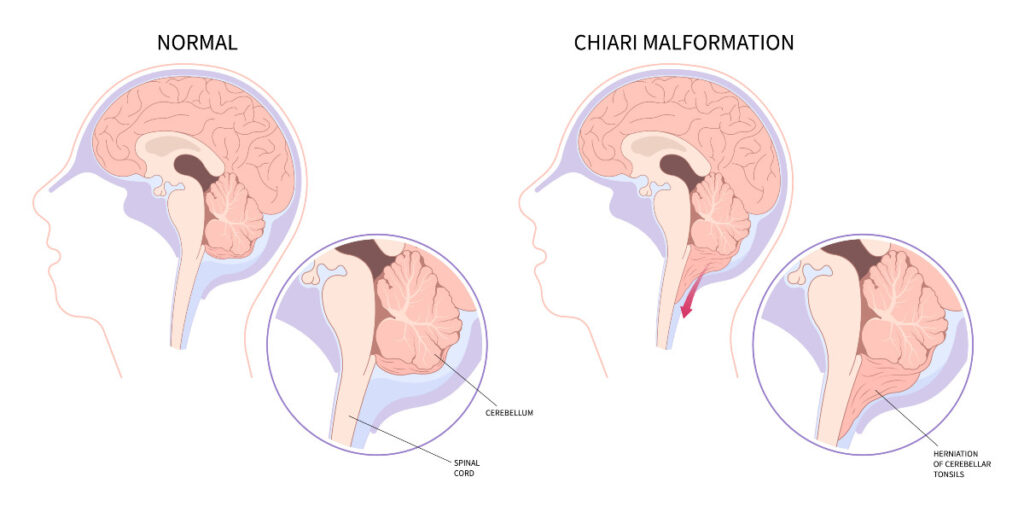


![Brain Under Pressure – A Guide to Understanding Intracranial Hypertension [Achive #2]](https://chiaribridges.org/wp-content/uploads/2019/12/Woman_Up-with-headache_AS177290930.jpg)
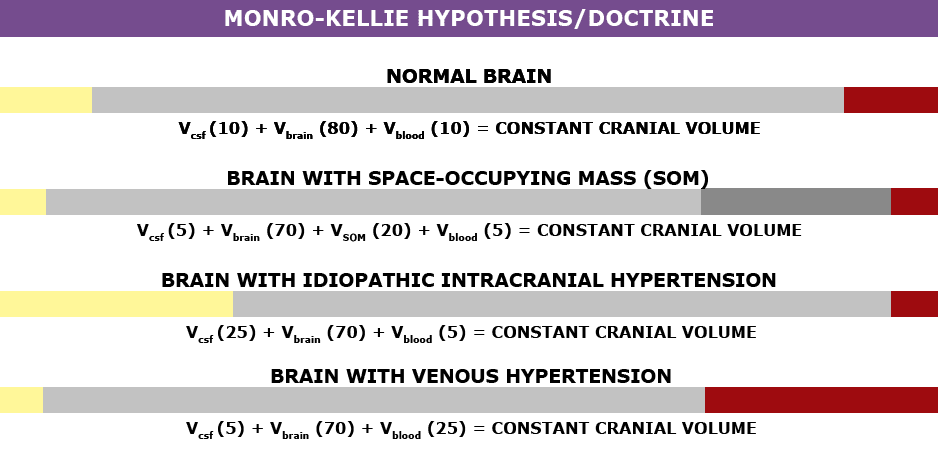



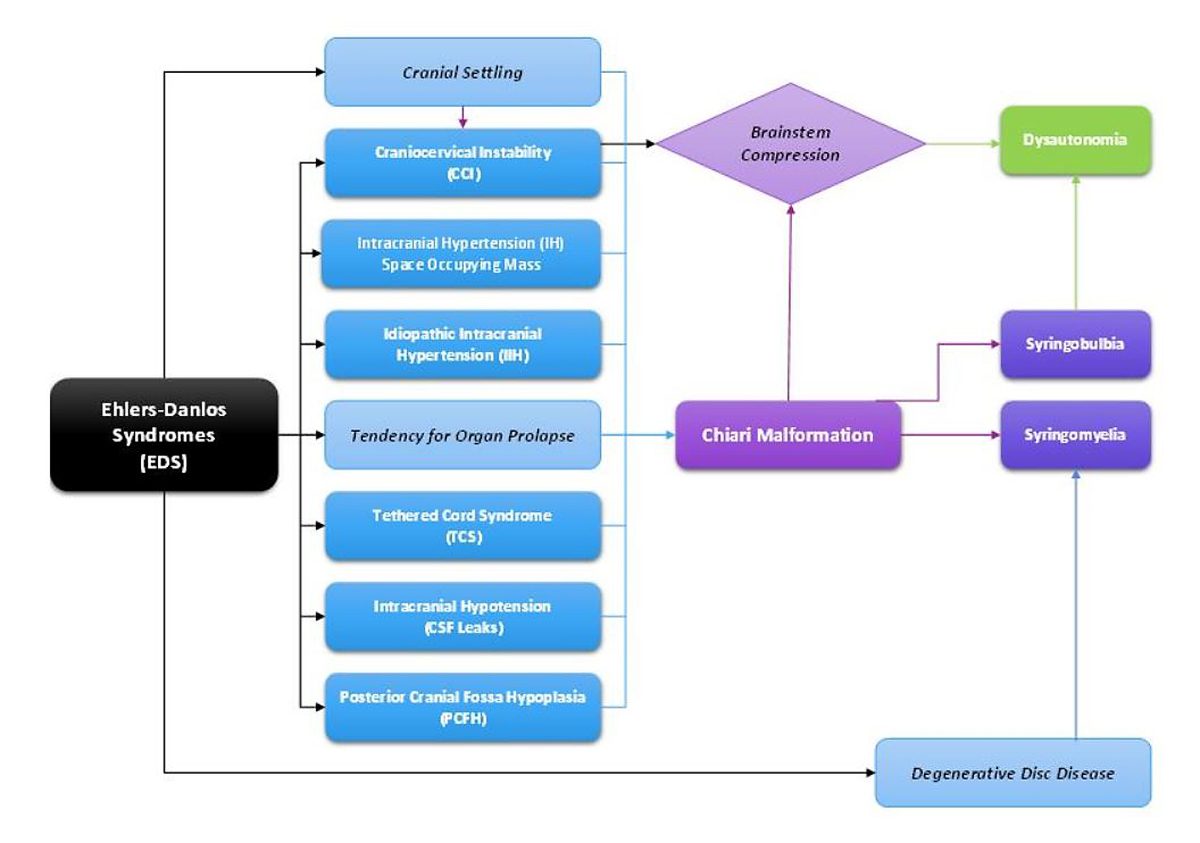



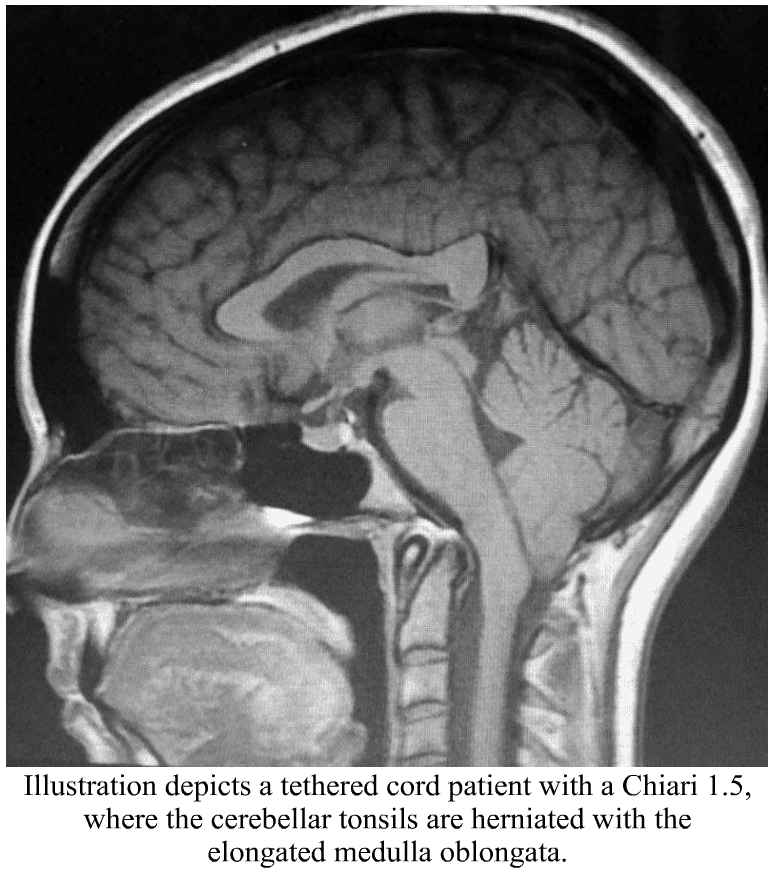 Chiari Malformation has many conditions that can be associated with it (comorbid conditions) and sometimes those comorbid conditions can be at the root cause (etiological cofactor) or one of the causes along the way (pathological cofactor) to the tonsils being as low as they are (making the Chiari “secondary” to one or more “other” conditions). Tethered Cord Syndrome (TCS) is one of those pathological conditions.
Chiari Malformation has many conditions that can be associated with it (comorbid conditions) and sometimes those comorbid conditions can be at the root cause (etiological cofactor) or one of the causes along the way (pathological cofactor) to the tonsils being as low as they are (making the Chiari “secondary” to one or more “other” conditions). Tethered Cord Syndrome (TCS) is one of those pathological conditions.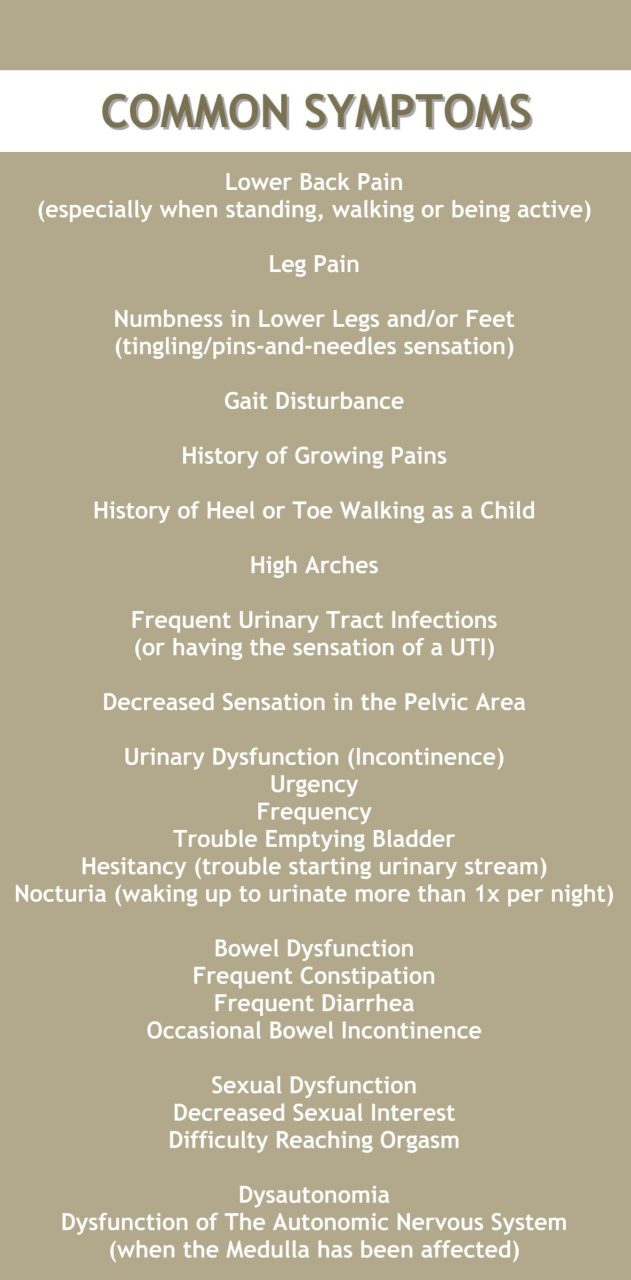
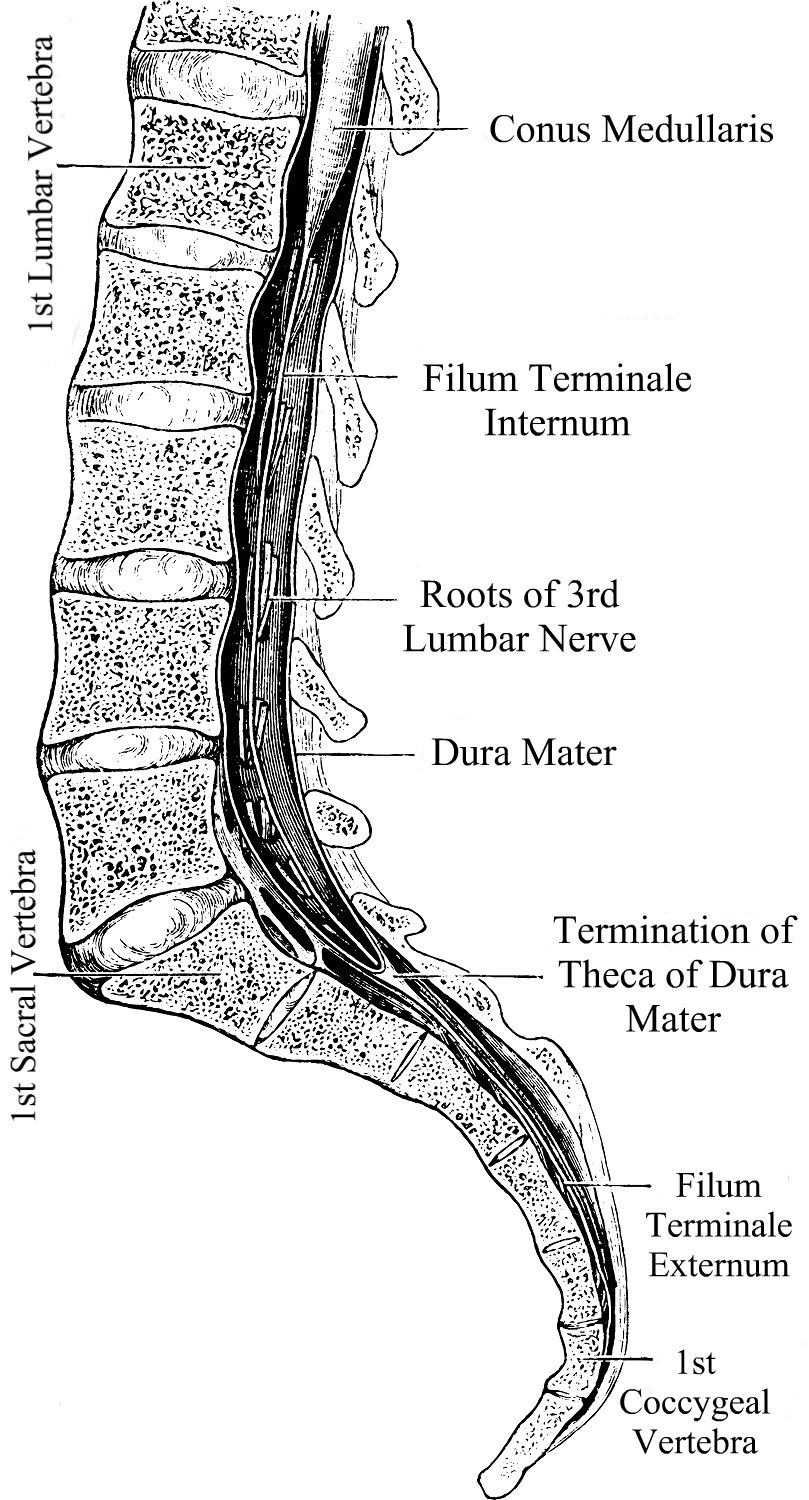 What We Recommend
What We Recommend 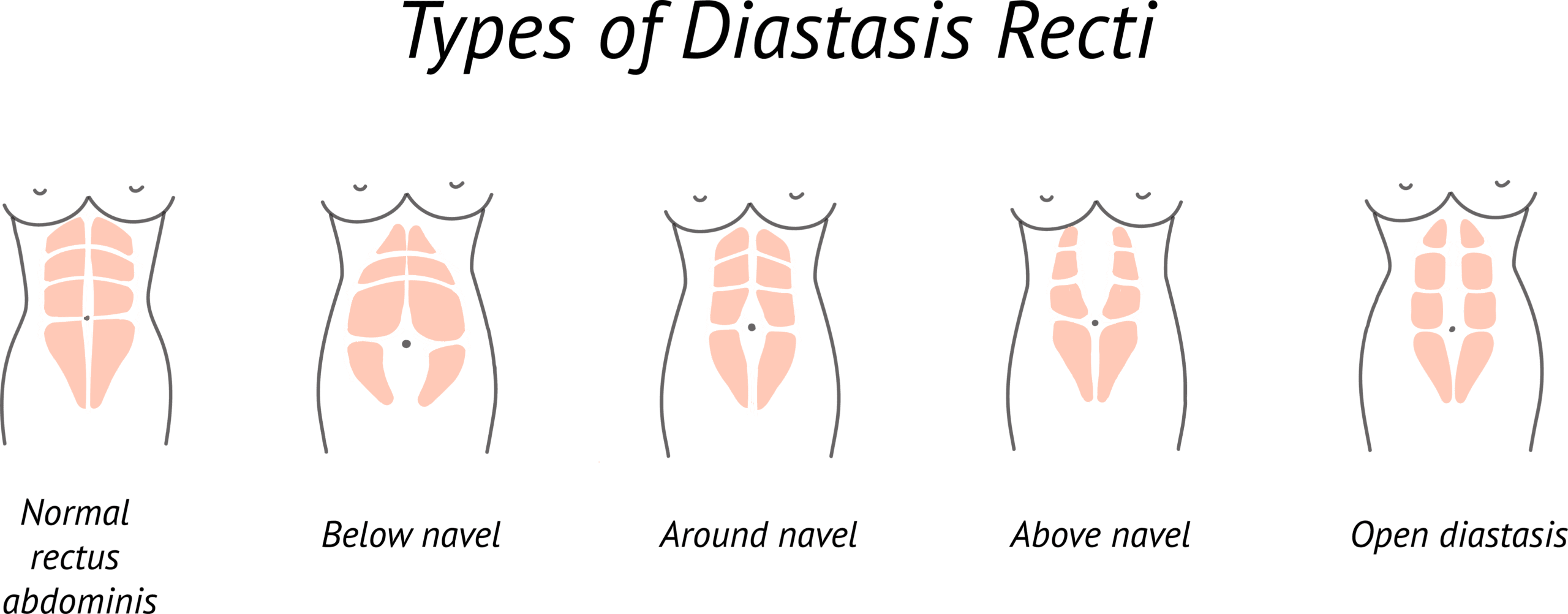
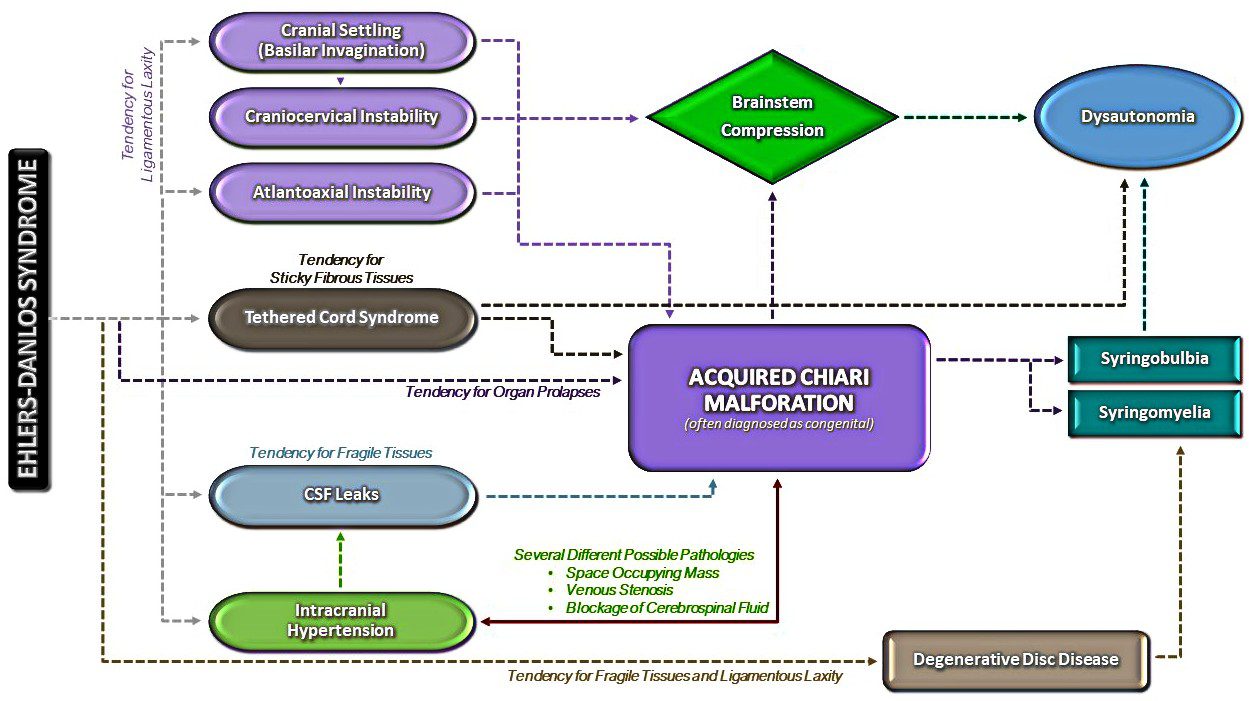

 It leaves a hole in the hearts of the Chiari community because, even as dysfunctional as we are sometimes, we know we’re all in this together!
It leaves a hole in the hearts of the Chiari community because, even as dysfunctional as we are sometimes, we know we’re all in this together!  Her husband has had days where he was so petrified at the thought of losing her. Sometimes that fear manifested as anger and frustration, but it wasn’t her that he was really mad at; He was mad at the Chiari that was taking his wife from him. He regretted those words from the very minute that he gazed upon her eyes as she heard them. He couldn’t make her forget those words, they pierced her soul too deeply, so he internally committed to just try and show her why he loves her. Despite his frustrations with the situation, he admired this amazingly strong woman who was facing more pain than he could ever understand. He’s cried out to God privately for this soul mate that he committed to so many years ago. He feared losing her and he did not know how he could ever hold everything together like she did, but he had to try because there was so much was on his shoulders. He never talked much about the weight he carried in it all, because he knew what she was facing was already more than she could handle. So, he learned to grieve as silently as he could – to understand what he could, to empathize as he could, to remain as strong for her and the family as best as he could.
Her husband has had days where he was so petrified at the thought of losing her. Sometimes that fear manifested as anger and frustration, but it wasn’t her that he was really mad at; He was mad at the Chiari that was taking his wife from him. He regretted those words from the very minute that he gazed upon her eyes as she heard them. He couldn’t make her forget those words, they pierced her soul too deeply, so he internally committed to just try and show her why he loves her. Despite his frustrations with the situation, he admired this amazingly strong woman who was facing more pain than he could ever understand. He’s cried out to God privately for this soul mate that he committed to so many years ago. He feared losing her and he did not know how he could ever hold everything together like she did, but he had to try because there was so much was on his shoulders. He never talked much about the weight he carried in it all, because he knew what she was facing was already more than she could handle. So, he learned to grieve as silently as he could – to understand what he could, to empathize as he could, to remain as strong for her and the family as best as he could. Her children have learned to grieve in silence as well. They learned to face life and all the obstacles they faced without making waves at home. How could they? They saw the pain that flared when things had stressed her in the past. They didn’t want to cause that again. They longed having the mom that they used to have, the mom with the strength to climb every mountain with them, the mom that made every challenge in life seem conquerable. They admired her strength and never understood how they could admire so much in her yet hate the fact that she wasn’t always there for them anymore. Even when she so desperately tried to be there the brain fog often dominated and took over the conversation entirely, this conversation that she probably wouldn’t remember for long. They resented her for it but knew that it wasn’t her fault. Like everyone else that loved her the most, they said so many things that they regretted. They knew that they often came across like they hated her, but the real truth was there was no one in the world that they longed for more. They’ve always hated seeing her in pain, yet her pain served as a constant reminder of the future that they feared in their future. They remember when she told them about the hereditary nature of the genes passed on to them, with tears in her eyes. Would they have what she had? Would they become as symptomatic? Would they have the courage to fight it as valiantly as she did? Should they have children one day? The reasons for concern were endless.
Her children have learned to grieve in silence as well. They learned to face life and all the obstacles they faced without making waves at home. How could they? They saw the pain that flared when things had stressed her in the past. They didn’t want to cause that again. They longed having the mom that they used to have, the mom with the strength to climb every mountain with them, the mom that made every challenge in life seem conquerable. They admired her strength and never understood how they could admire so much in her yet hate the fact that she wasn’t always there for them anymore. Even when she so desperately tried to be there the brain fog often dominated and took over the conversation entirely, this conversation that she probably wouldn’t remember for long. They resented her for it but knew that it wasn’t her fault. Like everyone else that loved her the most, they said so many things that they regretted. They knew that they often came across like they hated her, but the real truth was there was no one in the world that they longed for more. They’ve always hated seeing her in pain, yet her pain served as a constant reminder of the future that they feared in their future. They remember when she told them about the hereditary nature of the genes passed on to them, with tears in her eyes. Would they have what she had? Would they become as symptomatic? Would they have the courage to fight it as valiantly as she did? Should they have children one day? The reasons for concern were endless. Depending on when she became symptomatic, her parents have likely spent endless days and nights in hospitals and emergency rooms. They’ve spent years learning all they could and even learned to recite her diagnoses with detailed explanations because they’d became so accustomed to these conditions that so few doctors could pronounce, much less treat. For years they made sure to always have her complete medical chart in hand with official documentation, in case they were challenged by a medical professional or anyone dared to call their daughter “a drug seeker” or “psychosomatic.” They spent countless hours trying to dull the tortuous pain they saw her go through, and spent many more hours researching creative home remedies to give her a sense of relief, even if it was only momentary. There were times they prayed for God to just go ahead and take her, so she wouldn’t be in anymore pain; and then felt guilty for even thinking it. Then one day the screaming stopped, the pain was gone, but with it so went their daughter.
Depending on when she became symptomatic, her parents have likely spent endless days and nights in hospitals and emergency rooms. They’ve spent years learning all they could and even learned to recite her diagnoses with detailed explanations because they’d became so accustomed to these conditions that so few doctors could pronounce, much less treat. For years they made sure to always have her complete medical chart in hand with official documentation, in case they were challenged by a medical professional or anyone dared to call their daughter “a drug seeker” or “psychosomatic.” They spent countless hours trying to dull the tortuous pain they saw her go through, and spent many more hours researching creative home remedies to give her a sense of relief, even if it was only momentary. There were times they prayed for God to just go ahead and take her, so she wouldn’t be in anymore pain; and then felt guilty for even thinking it. Then one day the screaming stopped, the pain was gone, but with it so went their daughter.
 Like any marriage, we’ve had our rocky moments. We’ve both showed our ugly sides more than we like to admit. I’m not sure when he changed, but somehow along the way in our 27 years of marriage, my husband morphed into this amazing man who is EXACTLY what I need in every way!
Like any marriage, we’ve had our rocky moments. We’ve both showed our ugly sides more than we like to admit. I’m not sure when he changed, but somehow along the way in our 27 years of marriage, my husband morphed into this amazing man who is EXACTLY what I need in every way! relieving all of my symptoms, but never in a million years did we think that decompression would open Pandora’s Box on my need for surgeries. From 2012-2015 I needed seven additional surgeries. Each surgery had its own recovery and complications. And with each additional surgery, I became increasingly dependent on my husband for help, but not once did he complain. This was affecting his life too, but not once did he concentrate on that. Not once did he think of it as being unfair to him to have to care for me, even though it really was. I’m now covered with scars on my left side from my neck to my groin, one night he raised my pajama shirt and gazed intensely upon them. He started kissing them. When he got to the scars covering my stomach, I pushed him away and with tears in my eyes, I told him that I wasn’t comfortable with him touching me there. He looked me in the eyes and told me that he didn’t see me the way that I see myself. He said that when he sees my scars, he’s reminded of all that I’ve had to fight through and what a strong woman he’s married to. “I wish that you could see yourself the way that I see you,” he exclaimed. All my insecurities just melted with his words of affirmation.
relieving all of my symptoms, but never in a million years did we think that decompression would open Pandora’s Box on my need for surgeries. From 2012-2015 I needed seven additional surgeries. Each surgery had its own recovery and complications. And with each additional surgery, I became increasingly dependent on my husband for help, but not once did he complain. This was affecting his life too, but not once did he concentrate on that. Not once did he think of it as being unfair to him to have to care for me, even though it really was. I’m now covered with scars on my left side from my neck to my groin, one night he raised my pajama shirt and gazed intensely upon them. He started kissing them. When he got to the scars covering my stomach, I pushed him away and with tears in my eyes, I told him that I wasn’t comfortable with him touching me there. He looked me in the eyes and told me that he didn’t see me the way that I see myself. He said that when he sees my scars, he’s reminded of all that I’ve had to fight through and what a strong woman he’s married to. “I wish that you could see yourself the way that I see you,” he exclaimed. All my insecurities just melted with his words of affirmation.
 Palliative Care (pronounced “pal-lee-uh-tiv” care) is a subspecialty of medical care, where an interdisciplinary team of professionals (both medical and social) are committed to helping provide “relief from symptoms and stress” for patients with serious, life-altering illnesses, and their families.
Palliative Care (pronounced “pal-lee-uh-tiv” care) is a subspecialty of medical care, where an interdisciplinary team of professionals (both medical and social) are committed to helping provide “relief from symptoms and stress” for patients with serious, life-altering illnesses, and their families.  Misconceptions Surrounding Palliative Care:
Misconceptions Surrounding Palliative Care:  Primary Care Doctors (who are supposed to be offering referrals to Palliative Care for their patients with serious medical conditions) often fail to fully understand the spectrum of Palliative Care. Because of their faulty understanding, most of us are never offered Palliative Care, and when we request it, we are often told that it is equivalent to hospice care or set aside for hospice patients, and therefore they believe that we do not qualify. THEY ARE WRONG!
Primary Care Doctors (who are supposed to be offering referrals to Palliative Care for their patients with serious medical conditions) often fail to fully understand the spectrum of Palliative Care. Because of their faulty understanding, most of us are never offered Palliative Care, and when we request it, we are often told that it is equivalent to hospice care or set aside for hospice patients, and therefore they believe that we do not qualify. THEY ARE WRONG!