2 cups kale, washed, ribs removed, and roughly chopped
4 cups 50/50 Spinach/Spring Mix salad greens
8 radishes, thinly sliced
½ cucumber, sliced into half moons
¼ red onion, thinly sliced
½ cup fresh blueberries
1 medium carrot, shaved with a vegetable peeler or grated with a cheese grater
1 medium avocado, sliced
DIRECTIONS:
In a blender, combine all dressing ingredients. Blend on high speed about 20 seconds, or until dressing is smooth and emulsified. Taste dressing and add more honey if it is too tart. The sweetness may vary depending upon the ripeness of your blueberries and the quality of your balsamic vinegar. Set aside at room temperature.
Place walnuts in a food processor and pulse until walnuts are ground, resembling course breadcrumbs. Avoid the temptation to leave the food processor on high, as this can result in a nut butter. Mix ground walnuts, onion and garlic powders, salt and pepper in a medium bowl or pie plate. In a separate medium bowl or pie plate, whisk together eggs and water.
Cut each chicken breast in half by thickness by laying the breast on a cutting board and pressing down on it with the palm of one hand. Using a chef’s knife in your other hand, hold the blade parallel to the cutting board and slice through the thickness of the breast, using a sawing motion. Repeat with the other chicken breast. You should now have four fairly thin chicken cutlets. Pat them dry with a paper towel.
Heat your chosen cooking oil on medium heat in a large, nonstick skillet. If your skillet is not large enough to accommodate all four cutlets, use half the oil at a time and work in two batches. Dip each cutlet in the egg wash, then the walnut mixture, pressing the walnuts onto the chicken. Place chicken in heated pan and cook approximately 3-4 minutes on each side, until walnut coating is deep golden brown and chicken is cooked through. Remove to a CLEAN cutting board to rest. Allow to rest and cool for five minutes, then cut into ½-inch slices.
While chicken is resting, assemble your salad, by combining all the ingredients except avocado in a large bowl. Divide the salad into four bowls and top each bowl with a sliced walnut-crusted chicken cutlet and ¼ of the sliced avocado. Drizzle prepared vinaigrette over chicken and salad and serve immediately. Leftover dressing can be stored in the refrigerator, but will be best if you let it return to room temperature before serving.
Despite the pain we face on a daily basis, that our doctors so often ignore…
Despite the anger that builds towards a medical system that is relatively clueless about our conditions…
Despite the frustrations we face when those we love fail to understand what we’re going through…
… Despite it all, hope remains!
“They tried to bury us. They didn’t know we were seeds.”
There is little easy about the Chiari fight (and that of its co-morbid conditions), but it is easy to lose hope! The thing about that however, is if you look at the complexities of our bodies and the conditions we face, one thing is for sure, we weren’t created for easy! Coping with conditions like Chiari Malformations, Ehlers-Danlos Syndromes, and their many ugly friends can be a very daunting task that we all have to face. There are many challenges, including chronic pain that can be severe, fatigue that can be debilitating, the fight with doctors for proper diagnosis and treatment, the fight with loved ones to be understood and supported, and the general lack of awareness of these conditions in the public. It is easy to lose sight of the light at the end of the tunnel. But, even with all the hardships we face, there is a lot to still be hopeful about.
Education & Research One of the most frustrating aspects of dealing with Chiari and its comorbidities is the lack of education within the medical community. There is little more disconcerting than walking into a doctor’s appointment and being asked to spell your condition, so the doctor can Google it. These appointments often end in tears because the doctor has absolutely no clue about our condition, but this is improving. Just ten years ago, few of the doctors we encountered had heard of Chiari Malformation, we had to explain it to almost every doctor we came across, regardless of their specialty. This is happening far less now. While there are still many misconceptions that medical professionals tend to have about these conditions, many have a general level of familiarity now. That means we are making real progress and the future is looking brighter. In a recent webinar on Chiari, Complex Chiari and Craniocervical Instability, Complex Chiari expert, Dr. Paolo Bolognese shared the following:
In reference to the association between EDS and Complex Chiari, Dr. Bolognese shared that he stumbled upon the association in 2002 during office visits, when he saw a half dozen patients in a 2-week period diagnosed with both. After consulting colleagues and experts in genetics and connective tissue disorders, Dr. Bolognese and his colleague, Dr. Milhorat, conducted a pilot study of the association and published their findings in a major neurosurgical journal in 2006. These findings were met with much skepticism among even the world’s top Chiari experts. In 2017, however, at the XXIX ASAP Conference on CM1, Dr. Bolognese submitted a questionnaire to these top experts. 63 experts from 4 countries responded. 77.5% agreed that there is an association between EDS and CM1. 99.5% agreed about the existence of Complex Chiari. On this fight to get other experts to see the connection, Dr. Bolognese said, “Science does not have a linear behavior. It goes in accelerations, stops, accelerations, stops, some steps backwards, some steps forward. So, it took 12 years to convince most of the leading experts in our field. It will take 12 more years to convince the ‘regular’ neurosurgeons. It will take 12 more years to convince primary care physicians.”
While this delay in translating research and scientific discovery into medical practice is frustrating for us as patients, there are also some great reasons to be hopeful. First, there are doctors who have dedicated their careers to helping us find answers and improving our quality of life in the meantime. These doctors are willing to put their professional reputations on the line and face the critics to make improvements in our treatment outcomes. Second, the experts are being convinced, and as more experts come to believe in what we, the patient community, already know to be true, it is more likely that younger generations of doctors and researchers will want to get involved in these areas of research. While many of us are suffering and fighting for care by physicians who fully understand the complexities of our conditions, progress is being made that will likely revolutionize the future of patient care.
In addition to this little snapshot into the experts’ world, anyone who has spent any time in online support groups over the last decade can tell you that patients are getting diagnosed sooner, tested for comorbid conditions more often, and are having better surgical outcomes because they are better informed and are asking all the right questions of their doctors. This trend is likely to continue as patients now have better access to pertinent research information through a wide variety of educational materials offered online by Chiari and EDS non-profit organizations. It is finally OUR time and each of us can do our part to make the most of it, by educating ourselves and sharing information with others, as well as supporting the organizations that make this information available to us.
Support Thanks to the worldwide availability of the internet and social media, support is easier to access and is more abundant than ever before. Patients and caregivers alike can now find a wide variety of support groups for these conditions on a variety of social media platforms. Groups range from small and intimate, to large and very active, and there is a fit for practically any personality. There are groups for women only, men only, teens only and parents only. There are groups focused on laughter and those focused on hobbies like gaming or crafting. Some groups focus on support, while others focus on information, and some do an excellent job at both. There are international groups where you can interact with other patients from around the world, and there are local groups where you can potentially meet people in your own town or surrounding area. There are also numerous in person support group meetings where you can meet fellow patients, attend educational lectures, participate in awareness activities, and much more. Interacting with others who are enduring similar struggles is not only an opportunity to feel less alone and more validated, it is also an opportunity to help others and even potentially form lifelong friendships.
Awareness The patient community has made great strides in raising awareness for Chiari and related disorders. Between individuals sharing awareness materials on social media, patients reaching out to local media to share their stories and organizations hosting awareness walks, much needed attention and information is getting out to the public. While we still have a long way to go in making Chiari a household name, we are making progress toward it. You can join in these efforts by getting intentional about awareness! What has helped you, might help others!
Creating Our Own Hope We have been a neglected community for far too long. We have been ignored, dismissed, and sometimes even abused. We have had doctors laugh in our faces, call us crazy, and even accuse us of making things up. It often leaves us feeling hopeless, like there’s nowhere left to turn, but we are standing up and demanding better care. We are demanding that our healthcare professionals educate themselves and study the most recent research. We are demanding that our voices be heard and that we are taken seriously. Although there has been some progress, our fight is far from over. It is just beginning, and we refuse to sink into the shadows because we are mighty warriors who will fight for what we need! When necessary, we will create our own hope! As the old Mexican proverb goes, “They tried to bury us. They didn’t know we were seeds.” Our community is growing every single day and there is a need now, more than ever, to stand up not only for ourselves, but those among us who are vulnerable and need us to do it for them. Please, whether you are a patient yourself, a caregiver, a spouse, family member or friend to someone who is suffering, find your inner warrior and join us in this fight!
[wpedon id=”4396″ align=”center”]
Overview: Complications Associated With A Chiari Decompression
From Intracranial Hypertension (formerly known as Pseudotumor Cerebri), Hydrocephalus, Tethered Cord Syndrome, to conditions related to the presence of a connective tissue disorder, such as Ehler’s-Danlos Syndrome, the primary reason for post-decompression complications seen in the Chiari Patient Community continues to be largely related to undiagnosed and untreated comorbid conditions. Time and time again, we see decompression failure, or a recurrence of symptoms after decompression, because there are other underlying conditions that need to be addressed. For this reason, we strongly recommend that patients get evaluated for the possibility of these known comorbid conditions before undergoing decompression surgery, unless circumstances require emergency surgery. (More information about the testing we recommend can be found in “The Treatments” article). Potential complications of decompression surgery may vary, depending upon the specific technique used, such as whether a duraplasty is performed, and how much bone is removed during a suboccipital craniectomy. The most common complications are infection, CSF leak, and Pseudomeningocele in adult patients.
INFECTIONS
Surgical site infections:
A surgical site infection is a risk of any surgery. While hospitals and surgical staff strive to maintain a sterile environment, hospitals are known for harboring pathogens, including many that are antibiotic resistant. Patient factors, including diabetes, age, being overweight, and being a smoker can also increase a patient’s risk of developing a post-operative infection.[1] Antibiotics are typically given post-surgically (and sometimes before surgery) in order to reduce the risk of infection. Some infections require wound revision surgery, to remove pus and infected tissue in order to improve healing.
Meningitis is an additional surgical risk when the dura is opened during a decompression. It is characterized by inflammation of the meninges, the linings of the brain. There are three main types of meningitis: aseptic, bacterial and chemical.
♦ Aseptic Meningitis is by far the most common type, and is generally less severe than the bacterial type. Most cases of aseptic meningitis are caused by viruses, but may rarely be fungal, autoimmune, parasitic or drug-induced.[2] The treatment for aseptic meningitis is usually supportive care.[3] Chemical meningitis is also a risk any time surgery or other procedures or treatments are performed on the brain or spine.[4]
♦ Bacterial Meningitis is much more serious and can be life threatening. Three types of bacteria cause most cases: streptococcus pneumoniae, Group B streptococcus, and Neisseria meningitidis. Typical treatment includes antibiotics and supportive care.
CSF LEAKS
Duraplasty leak:
Post-decompression CSF leaks are a risk of decompression surgery whenever the dura is opened. The risk of a CSF leak dramatically increases with the presence of untreated hydrocephalus[5], intracranial hypertension (IH)[6], and connective tissue disorders, such as Ehlers-Danlos Syndrome. Nationwide statistics indicate that the risk of a CSF leak post-duraplasty is 10-15%. However, some surgeons report a significantly lower incidence of CSF leaks in their patients.[7] The use of biologic glue to seal the dural suture line has greatly reduced the incidence of post-duraplasty CSF leaks. A common sign of a leak is clear fluid leaking from the incision site.
Pseudomeningocele:
A pseudomeningocele is a type of CSF leak, where the leak creates a pocket in the muscles in the back of the neck. It is one of the most common complications of duraplasty. While some surgeons have managed to keep the incidence of pseudomeningocele low in their patients, some report an incidence as high as 18%.[8] A study at Vanderbilt University at 2013 showed that the development of a pseudomeningocele after decompression significantly reduced the benefit of decompression at one-year post-op on pain, disability and quality of life.[9] A smaller pseudomeningocele may re-absorb on its own. However, with large and persistent PM’s, the duraplasty may adhere to the cerebellar tonsils, blocking flow and making a revision surgery more difficult. There is much debate among neurosurgeons as to whether doing routine duraplasty as part of decompression outweighs the risks. Some argue that duraplasty increases the risk of complications, while others say that failure to perform duraplasty often results in inadequate decompression, reduced benefit, and the need for additional surgeries. Some experts argue that duraplasty using the patient’s own pericranial tissue and using water-tight sutures and biologic glue minimizes the risk of a leak and makes routine duraplasty the best option for most patients. A squishy pocket of fluid is often seen near the base of the skull and a PM can be confirmed and monitored with an MRI. In some cases, a surgeon may try draining the pocket of fluid with a needle and syringe.
BLEEDING AND ANESTHESIA-RELATED COMPLICATIONS
Excessive Blood Loss:
Excessive blood loss is a risk of any major surgery, but can be minimized by a careful surgical technique. Patients with connective tissue disorders may have an increased risk of bleeding complications, due to fragile blood vessels, particularly with vascular EDS or vascular crossover symptoms. Cessation of blood-thinning medications, such as warfarin, aspirin and NSAIDS also reduces the risk of bleeding.
Anesthesia Risks:
While risks of general anesthesia are quite low, the risk may be higher if you or someone related to you has had previous adverse interaction to general anesthesia. Some EDS patients are also prone to anesthesia issues, such as requiring more anesthesia or ineffectiveness of local anesthetics. Therefore, it is important to inform your anesthesiologist of your pertinent medical history.[10]
BONY REGROWTH
Regrowth of the bone removed during decompression is a risk associated with the pediatric patient population, particularly patients under the age of 2. Surgeons have reported as much as a 50% incidence of bony regrowth in patients under the age of 5, and as much as 80% in patients under age 2. Regrowth of bone may result in the need for future surgery.[5]
While Craniocervical Instability is not uncommon among those with connective tissue disorders, it is pretty rare in the general population. However, aggressive bone removal during decompression surgery can create an unstable craniocervical junction. It is important to discuss with your surgeon how much bone they plan to remove, and the risks and benefits of laminectomy, particularly if you also have a connective tissue disorder, which increases your risk for developing instability.
CEREBELLAR SLUMPING (PTOSIS)
Cerebellar slumping (aka cerebellar ptosis) occurs as a result of too much bone being removed around the foramen magnum that there is no longer enough bone to support the weight of the cerebellum. The brain slumps downward toward the spine, re-herniating the cerebellar tonsils, and often compressing the cerebellum itself against the back of the skull and brain stem. This can often result in worse symptoms than the patient had before decompression. Surgical techniques have been developed to revise the decompression and provide more support to the cerebellum.[11]
Occipitalneuralgia is nerve pain, often accompanied by numbness and/or tingling, of the occipital nerve in the back of the head. It can be caused by compression of or damage to the occipital nerve. While the presence of a Chiari malformation itself can cause compression of the cranial nerves, including the occipital nerve, decompression surgery can also cause occipitalneuralgia. This can be due to compression of the nerve from the use of retractors to hold apart musculature during surgery, or the build-up of scar tissue around the nerve. More conservative treatment of occipitalneuralgia may include medications, such as lidocaine patches and medication that target nerve pain, physical therapy, cutaneous nerve stimulators, and nerve root blocks. Severe and persisting occipitalneuralgia may require surgical decompression of the nerve or occipital neurectomy, surgical removal of the occipital nerve.[12]
SCAR TISSUE AND ADHESIONS
Like with occipitalneuralgia and pseudomeningocele, the development of scar tissue and adhesions can cause symptoms to return or failure to relieve symptoms after a decompression surgery. Adhesions and scar tissue can develop wherever tissue is cut, including the dural graft, cauterized tonsils and the skin incision. Scar tissue and adhesion can inhibit or block CSF flow and often require revision surgery to remove the scar tissue. A careful selection of the graft material used for a duraplasty may reduce the risk of developing adhesions and scar tissue.[13]
DECOMPRESSION FAILURE
While perhaps technically not a complication, the failure rate of decompression surgery to alleviate symptoms deserves a mention here. While proper complications can often result in the failure of a decompression to relieve symptoms, or in fact, may make them worse than before decompression, even complication-free decompressions surgeries have a high rate of failure, as much as 40%, depending upon the study. Some reasons for decompression failure in the absence of the above-listed complications include failure to diagnose and treat comorbid conditions that may be causing symptoms, an inadequate decompression (failure to create enough space by removing bone and performing a duraplasty), and some or all of the symptoms being due to another cause, such as migraines. In cases of an inadequate decompression, a more aggressive decompression revision surgery may provide relief. In cases where a comorbid condition exists, that condition must be diagnosed and treated. However, there are still a small percentage of patients who do not get relief, even with further decompression and other treatments. The reason for this is not clearly understood.[5]
9 Parker, S. L., et al. “Effect of Symptomatic Pseudomeningocele on Improvement in Pain, Disability, and Quality of Life Following Suboccipital Decompression for Adult Chiari Malformation Type I.” Journal of Neurosurgery., U.S. National Library of Medicine, Nov. 2013, <www.ncbi.nlm.nih.gov/pubmed/24010974>.
One of the biggest hurdles a Chiari patient may face is that of simply being diagnosed. Some studies cite an average of 5 years between the onset of symptoms significant enough for a patient to seek medical care and the patient receiving an accurate diagnosis of Chiari Malformation. Sadly, however, online support groups and message boards are peppered with the stories of patients who went undiagnosed, or more often, misdiagnosed, for decades. Patients are frequently misdiagnosed with conditions such as Fibromyalgia, Multiple Sclerosis, ChronicFatigue Syndrome, Chronic Migraine, and various autoimmune disorders. Even more disturbing is the fact that in a study by Dr. Thomas Milhorat of over 300 patients diagnosed with Chiari, 59% had been diagnosed with a psychosomatic illness.[1] Diagnoses such as Hypochondriasis, Somatoform Disorder, Conversion Disorder, and a tricky little term some doctors use to disguise the fact that they believe their patient’s symptoms are “all in their head,” called ‘Functional Somatic Syndrome’ (which by definition does not necessarily imply a psychosomatic cause but are often interpreted by other medical professionals in that manner) are frequently written in patient’s medical records to account for their very real, medically explainable symptoms.[2] This often further undermines a patient’s efforts to find a diagnosis when they decide to try a new doctor, with their defiled medical records in tow, often without even realizing what has been written in their charts or what it actually means in ‘doctor speak.’
Diagnosis of Chiari Malformation is based upon the presence of Chiari symptoms, such as an occipital headache that is brought about or worsened by Valsalva maneuvers, neurological symptoms such as poor balance, numbness or tingling in the arms, weakness in the legs, etc. combined with the “gold standard” of imaging studies for Chiari, an MRI of the brain.[3] The MRI should show a tonsillar herniation that inhibits the normal flow of CSF fluid out of the Fourth ventricle of the brain and through the foramen magnum. When normal flow is in question, a CINE MRI may be conducted to determine how the CSF is flowing through the brain and upper spinal canal. There, are, however, controversial cases sometimes referred to as “Chiari Zero,” where no herniation exists, but interruption of flow and symptoms are present.[4]
So, with all these wonderful tests available, why is it so difficult to get a diagnosis? Well, first of all, most primary care physicians and neurologists alike are under-educated or outright miseducated about Chiari Malformation. It has always been presumed to be a relatively rare disorder, and with over 7,000 rare diseases known to modern medicine, medical schools cannot give a thorough education to medical students on everyone. However, since the advent and now fairly commonplace use of the MRI, it is becoming apparent that Chiari is not quite as rare as it was once thought to be. When a primary care physician is stumped by a patient’s complaints of headaches and neurological symptoms, it is only natural to refer that patient to a neurologist for evaluation. But even many neurologists are grossly uninformed about Chiari. Many patients, even with an MRI that shows a herniation, are told that their many varied symptoms can’t possibly be due to the herniation of their brain, even with numerous studies available which show otherwise. Some patients have even been told by neurologists and even neurosurgeons that “Chiari doesn’t cause headaches [pain].” In fact, most symptomatic patients experience severe headaches, nerve pain, and pain from related disorders such as Syringomyelia.
Furthermore, radiologists across the U.S. are using vastly different criteria from one another to determine whether a patient’s herniation constitutes a Chiari Malformation. Some are using criteria of a 3-5mm herniation, others a 7 mm herniation, and some are failing to look for a herniation altogether. The latest research, in fact, suggests that the size of the herniation does not matter at all. Some people with large herniations show no symptoms, while others with quite small herniations experience severe symptoms. Experts are now focusing more on whether the herniation blocks the normal flow of cerebrospinal fluid (CSF) in determining whether a patient may benefit from surgical intervention.
It is important to address the situation of “Incidental Findings” of Chiari Malformation. It is true that sometimes while having an MRI for an unrelated matter, a completely asymptomatic patient is found to have a Chiari Malformation. Unless this type of patient were to become symptomatic later, no treatment is necessary in these situations. However, if you look at radiology reports with a claim of ‘incidental finding of Chiari Malformation,’ you are likely to see that the reason mentioned for the imaging being done was to look for a cause of headaches or other known symptoms of Chiari. In these cases, these are absolutely not ‘Incidental Findings.’ Again, this is an example of the lack of education about Chiari.
For patients, the best piece of advice one can give on your road to diagnosis of your symptoms, whether due to Chiari or something else, is to trust yourself and never give up seeking answers. If you believe your symptoms are due to Chiari or that your MRI may have been misread, get a second opinion from a neurosurgeon that specializes in treating Chiari Malformation.
[wpedon id=”4396″ align=”center”]
References:
1 Milhorat, T H, et al. “Chiari I Malformation Redefined: Clinical and Radiographic Findings for 364 Symptomatic Patients.” Neurosurgery., U.S. National Library of Medicine, May 1999, <www.ncbi.nlm.nih.gov/pubmed/10232534>.
2 Mayou, Richard, and Andrew Farmer. “Functional Somatic Symptoms and Syndromes.” BMJ : British Medical Journal, BMJ, 3 Aug. 2002, <www.ncbi.nlm.nih.gov/pmc/articles/PMC1123778/>.
3 “The Chiari I Malformation.” Chiari I | Chiari & Syringomyelia Foundation (CSF), <csfinfo.org/education/physician-information/chiari-i/>.
4 Hofkes, S K, et al. “Differentiation between Symptomatic Chiari I Malformation and Asymptomatic Tonsilar Ectopia by Using Cerebrospinal Fluid Flow Imaging: Initial Estimate of Imaging Accuracy.” Radiology., U.S. National Library of Medicine, Nov. 2007, <www.ncbi.nlm.nih.gov/pubmed/17890352>.
Overview: Craniocervical Instability and Related Disorders
Craniocervical Instability and related pathologies of the craniocervical junction are an important topic for anyone diagnosed with Chiari 1 malformation. “Complex Chiari,” or the presence of craniovertebral abnormalities or instability in addition to the presence of cerebellar tonsillar herniation, is present in approximately one fourth of all cases of Chiari 1 malformation[1]. These cases usually involve the presence of a geneticconnective tissue disorder and are thought by experts to be the cause of most Chiari decompression failures[2]. When the doctor and patient alike are not knowledgeable about these conditions and the additional symptoms that often accompany them, these more complex cases are often treated with a standard decompression, which can actually weaken the stability of the craniocervical junction more, and result in an increase of symptoms rather than a clinical improvement. Understanding what signs and symptoms to look for that may indicate that your Chiari is more complex, is vital in receiving the appropriate treatment the first time. This is especially important considering that, according to Chiari expert Paolo Bolognese, M.D., “[with revision surgeries], the results are not as good as if you had done the posterior decompression well the first time.”[3]
Punjabi and White define instability as the “loss of the ability of the spine under physiological loads to maintain relationships between vertebrae in such a way that there is no damage or subsequent irritation of the spinal cord, (brain stem) or nerve roots, and in addition that there is development of deformity or incapacitating pain due to structural changes.”[4] This means that the ligaments and muscles that normally hold the spine together, are too weak or damaged to handle the normal range of motion and weight of anatomic structures. For example, in Craniocervical Instability, the neck is not strong enough to support the normal weight of the head, without elements of the spine moving in such a way that it causes pain or damage to the nervous system (spinal cord, brain stem, and even cranial nerves). The result is that the bones that make up the lower skull and upper spine get pushed out of their normal anatomic location and begin to impinge on or cause stretching of these parts of the nervous system.
Craniocervical Instability can result from or be exacerbated by a trauma, such as a severe whiplash injury. However, many cases of CCI are associated with some sort of connective tissue disorder, such as a heritable disorder of connective tissue (HDCT, like Ehlers-Danlos Syndrome or Marfan’s), or an autoimmune condition that affects the connective tissue (such as Rheumatoid Arthritis), or a few other rarer conditions that affect the integrity of bony structures in the skull and spine. Instability can result either from lax ligaments and other connective tissues, soft bones (also seen in HDCTs) or from something like pannus formation, where repeated rubbing together of the joints causes a build-up of granulated tissue around bony structures and changes the way certain bones lie in relationship to one another[5]. Craniocervical Instability can also result as a complication of Chiari decompression surgery, when too much bone is removed from the skull, resulting in the instability of the skull on the top of the spine[6].
In the patient community, the term “CCI” is often used in reference to both Craniocervical Instability and Atlantoaxial Instability (AAI). CCI is often used to refer to the commonly seen combination of issues with the craniocervical junction, that include the instability of the joints where the skull meets the C1 vertebrae (which is true CCI), the instability of the joints between C1 and C2 (true AAI), a retroflexed odontoid, pannus formation, and a kyphotic clivo-axial angle (which are all forms of basilar impression/invagination). But CCI really should refer to the movement of the skull with respect to the spine. This sliding is referred to as “translation” and is measured on dynamic imaging in millimeters. The pathological threshold for the degree of translation of the basion with respect to the odontoid process between flexion and extension is 2mm, and any amount of translation greater than 1mm is capable of producing symptoms7. Likewise, at the C1-C2 joint, instability in the form of AAI can cause an excessive uncovering of the joint facets. Facets are the surfaces of the vertebrae that articulate with next vertebra. An uncovering of the facets that exceeds 20% is considered pathological.
The occipito-atlantic joint allows for about half of the cervical spine’s ability to flex and extend (tilt forward and backward). Likewise, the atlantoaxial joint [the articulation between C1 (atlas) and C2 (axis)] accounts for about half of the cervical spine’s ability to rotate the head. Because of this, these vertebrae lack the same amount of stability as the remainder of the spine, and ligaments are largely responsible for their stability[8]. Therefore, ligamentous laxity, as seen in connective tissue disorders, make these areas of the spine particularly prone to pathologic instability. Symptoms of AAI may include visual changes, syncope (fainting) or near-syncopal episodes, dizziness, nausea, facial pain, difficulty swallowing, choking, respiratory issues, and upper cervical tenderness. These symptoms will usually improve with the use of a neck brace[9]. For patients with connective tissue disorders, as are seen in 12-20% of patients diagnosed with Chiari, dynamic imaging is very important in identifying potential instability. The ideal tests to diagnose CCI and AAI are an upright MRI with flexion and extension and a 3D CT with rotational views, respectively[10]. It is important to note that ventral brain stem compression may not be seen on traditional supine MR imaging, while it may be very evident on dynamic imaging.
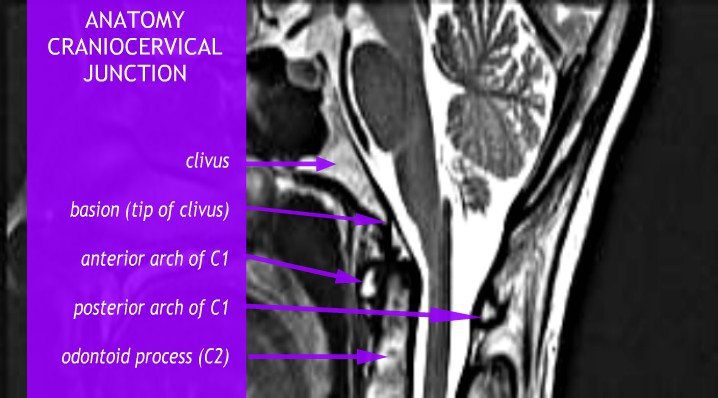
Basilar Invagination and Basilar Impression are also often seen with instability. They are almost identical to one another, and refer to upward displacement of the bones of the spine. However, technically, Basilar Invagination is caused by this deformation with normal bone, while Basilar Impression results from softening of bone[11]. For our purposes, this distinction is less important, but we will discuss any displacement in terms of “Basilar Invagination,” or “BI” for short. Forms of Basilar Invagination now include the prolapse of the odontoid process through the foramen magnum (the original condition described by the term), cranial settling, a kyphotic clivo-axial angle, and a retroflexed odontoid[12]. The kyphotic clivo-axial angle is an important and relatively easy measurement to indicate potential deformative stress on the brain stem. The clivus is a wedge-shaped bone that normally lies above and ventral to the top of spine. When it lies more horizontally, it creates a sharp angle that results in a bending of the brainstem. The odontoid peg (also called the odontoid process or the dens) is the part of the C2 vertebrae, or Axis, that the skull pivots upon, so named because of its tooth-like shape. A retroflexed odontoid occurs when the odontoid is bent backwards, often compressing the front of the brain stem. Other important measurements involving ventral brain stem compression for a kyphotic clivo-axial angle and/or retroflexed odontoid include the Grabb-Oakes and Harris measurements.
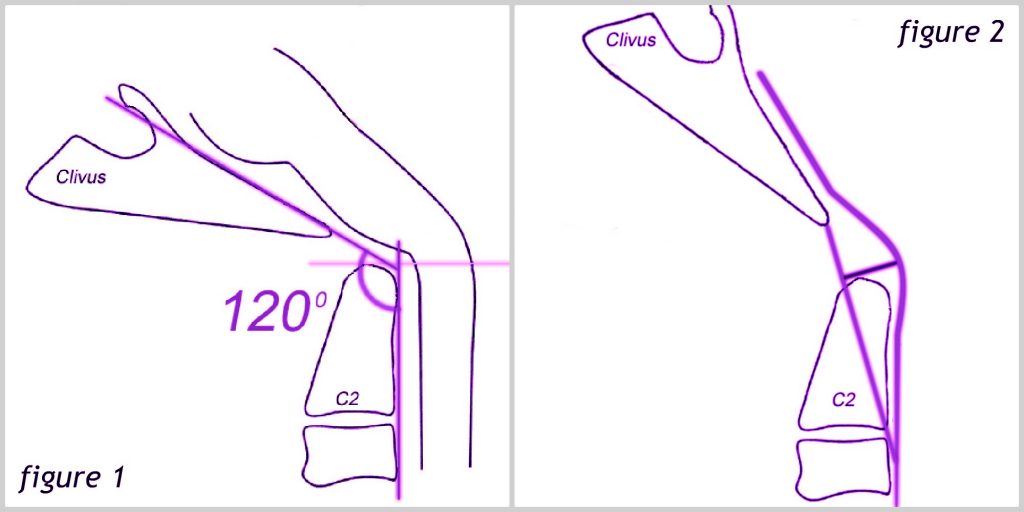
The clivoaxial angle is measured by drawing a line along the posterior (back, or when lying more horizontal, the top) side of the lower clivus and intersecting that line with a line drawn on the posterior side of the axis. If the angle created is less than 135°, it is considered pathological. Like instability, a kyphotic clivoaxial angle is often seen in patients with connective tissue disorders and degenerative rheumatoid disease[13]. See figure 1 below.
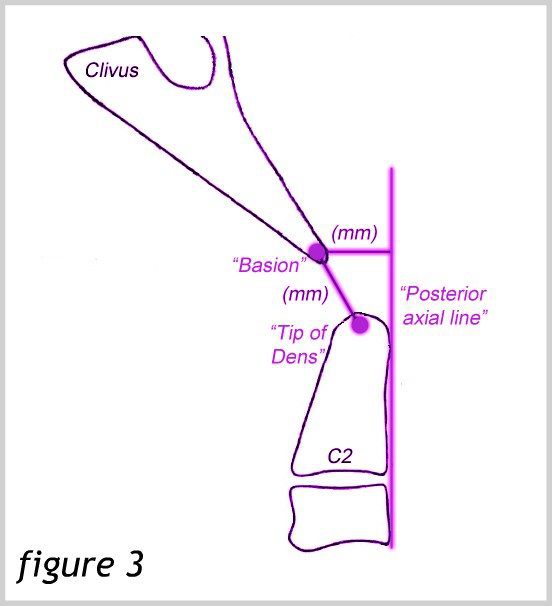
The Harris measurement is the distance between the basion and the PosteriorAxial Line. This distance should not be more than 12 mm. A measurement of more than 12 mm also denotes instability. This measurement can also be used to measure the translation between flexion and extension in dynamic imaging[14]. See Figure 3.
Symptoms of ventral brain stem compression can occur with various types of BI and instability. They may be referred to together as a “cervicomedullary syndrome” and may include[15]:
A heavy headache (often referred to as feeling like a “bobblehead” or feeling like the head is a “bowling ball”)
A Chiari-type pressure headache aggravated by Valsalva maneuvers (because these conditions, like Chiari, can also cause flow issues)
In more severe cases, non-epiform seizures have also been documented
In addition to producing significant pain and neurological symptoms, the compression and kinking of the brain stem can cause significant injury to the brain stem neurons by stretching the axons of the nerves to the point that they break and recoil, producing what are called “axon retraction bulbs” that can be seen on microscopic examination of the cells. The stress placed on the brain stem by both compressing and stretching simultaneously is much greater than the mere sum of these two mechanisms. Interestingly, during the flexion of the normal spine, it stretches 17% of its length. Research has shown that the axon of a giant squid fails when stretched to 20% if its length. Therefore, the normal motion of the human neck brings us very close to injuring our brain stem. Consequently, it only takes a slight alteration of our normal anatomy to cause injury to these delicate nervous tissues[16].
Treatment of Craniocervical Instability typically begins with more conservative medical management, such as neck bracing, activity limitation, physical therapy (including isometrics, sagittal balance, core strengthening and cardio), and pain management. Other causes of symptoms such as co-morbid conditions, multiple sclerosis, dystrophy, mitochondrial disorders, vitamin deficiencies and Lyme disease should be ruled out or treated. However, surgical intervention via a craniocervical fusion is indicated when the following criteria are met:
Surgeons and patients alike should consider surgery after medical management has been maximized and the patient has shown a positive response to neck bracing[10].
Various specific surgical techniques are applied in craniocervical fusions. A more common technique is the open reduction and fusion stabilization procedure. This procedure involves stabilizing the head with screws, making an incision that exposes the occiput through C2, and fixing plates to the occiput which attach to the C1 and C2 (and sometimes C3) vertebrae with rods. A newer technique adapted by Dr. Paolo Bolognese is using a less invasive Chiari decompression surgery known as MIST (minimally invasive subpial tonsillectomy) along with a fusion using screws placed in the occipital condyles. Although the dura is opened to partially resect the tonsils, a duraplasty is not done. Advantages of this procedure include a smaller incision, smaller hardware, less bone removal, and a thicker bone for which to insert screws in the occiput. Risks of both methods include vertebral artery injury, and a slightly increased risk for segmental instability below the fusion, along with the standard risks of any surgical procedure, such as bleeding, infection, and complications from anesthesia. Both procedures demand the hands of a very skilled and experienced surgeon because vital structures lie in and around the area. Using condylar screws may increase the risk of injury to major vessels, particularly in the hands of a less experienced surgeon. An important cranial nerve also lies just deep to the occipital condyles, making precise screw placement extremely important. This may limit the procedure in becoming more widely used, but the resulting fusion may be stronger, despite the reduced amount of hardware[17].
In the presence of a retroflexed odontoid, an open reduction, fusion and stabilization procedure may be enough to relieve ventral brain stem compression. However, in more severe cases, a further surgery called an odontoidectomy may be needed to remove the odontoid process. This surgery may be done through the mouth or the nose[18].
Every Chiari patient should be aware of hereditaryconnective tissue disorders and the signs and symptoms of Craniocervical Instability and Basilar Invagination. Many neurosurgeons do not evaluate their patients for these conditions prior to performing Chiari decompression surgery, often resulting in the need for revision surgeries and poor results. Being an educated patient can help you ask the right questions and insist on the proper evaluation and testing to avoid the pitfalls that many other patients have faced.
1 Bolognese, Paolo A, director. Surgical Techniques for Chiari Malformations. YouTube, American Syringomyelia Chiari Alliance Project, 16 Mar. 2015, <www.youtu.be/KfYmJnB6sPQ>.
2 Bolognese, Paolo A. “Modern Classification and Subclassification of Chiari Malformations.”YouTube, American Syringomyelia Chiari Alliance Project, 16 Mar. 2015, <www.youtu.be/ZQ9ZmquN-M0>.
3 Bolognese, Paolo A. “2016 ASAP CM/SM Conference – ‘Complex Posterior Fossa’ – Bolognese.” YouTube, American Syringomyelia Chiari Alliance Project, 7 Dec. 2016, <www.youtu.be/3jKH_DHadO8>.
4 Augustus A. White III, Manohar M. Panjabi, et al. “Clinical Biomechanics of the Spine.” By Augustus A. White III, <www.leomed.at/listhoscan/white_90.pdf>
5 The Pain Relief Foundation, The Pain Relief Foundation, <www.thepainrelieffoundation.com/craniocervical-instability/>.
7 Menezes, Arnold H. “Craniovertebral Junction Anomalies: Diagnosis and Management.”Seminars in Pediatric Neurology, vol. 4, no. 3, Sept. 1997, <www.sempedneurjnl.com/article/S1071-9091(97)80038-1/fulltext>.
8 Yang, Sun Y., et al. “A Review of the Diagnosis and Treatment of Atlantoaxial Dislocations.”Global Spine Journal, Georg Thieme Verlag KG, Aug. 2014, <www.ncbi.nlm.nih.gov/pmc/articles/PMC4111952/>.
9 Henderson, Fraser C., et al. “Neurological and Spinal Manifestations of the Ehlers–Danlos Syndromes.” American Journal of Medical Genetics Part C: Seminars in Medical Genetics, <www.onlinelibrary.wiley.com/doi/10.1002/ajmg.c.31549/full>.
10 Henderson, Sr. , Fraser C. “Neurological Management of Hereditary Disoders of HypermobilityConnective Tissue Disorders.” Ehlers-Danlos Society Annual Conference 2015. Ehlers-Danlos Society Annual Conference 2015, 14 Aug. 2015, Baltimore, <www.ehlers-danlos.com/2015-annual-conference-files/Henderson_0.pdf>.
12 Kim, Louis J., et al. “JNS JOURNAL OF Neurosurgery OFFICIAL JOURNALS OF THE AANS since 1944.” Treatment of Basilar Invagination Associated with Chiari I Malformations in the Pediatric Population: Cervical Reduction and Posterior Occipitocervical Fusion | Journal of Neurosurgery: Pediatrics, Vol 101, No 2, Nov. 2004, <www.thejns.org/doi/abs/10.3171/ped.2004.101.2.0189?url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org&rfr_dat=cr_pub%3Dpubmed>.
13 Henderson, Sr. , Fraser C. “Cranio-Cervical Instability in Patients with Hypermobility Connective Disorders.” OMICS International, OMICS International, 18 Apr. 2016, <www.omicsgroup.org/journals/craniocervical-instability-in-patients-with-hypermobility-connective-disorders-2165-7939-1000299.php?aid=71754#11>.
14 Bono, C M, et al. “Measurement Techniques for Upper Cervical Spine Injuries: Consensus Statement of the Spine Trauma Study Group.” Spine., U.S. National Library of Medicine, 1 Mar. 2007, <www.ncbi.nlm.nih.gov/pubmed/17334296>.
15 Henderson, Sr. , Fraser C. “Diagnosis and Treatment of Craniocervical Instability in the Chiari Patient.” Chiari and Syringomyelia Foundation Educational Lecture. 20 July 2011, Greater Metropolitan Washington Area, Greater Metropolitan Washington Area, <www.youtu.be/U33T8JFXvk0>.
16 Henderson, F C, et al. “Neuropathology of the Brainstem and Spinal Cord in End Stage Rheumatoid Arthritis: Implications for Treatment.” Annals of the Rheumatic Diseases, U.S. National Library of Medicine, Sept. 1993, <www.ncbi.nlm.nih.gov/pmc/articles/PMC1005138/>.
17 Bolognese, Paolo A. “Surgical Techniques for Chiari Malformations.” YouTube, American Syringomyelia Chiari Alliance Project, 16 Mar. 2015, <www.youtube.com/watch?v=KfYmJnB6sPQ>.
18 Hwang, Steven W., et al. “C1–C2 Arthrodesis after Transoral Odontoidectomy and Suboccipital Craniectomy for Ventral Brain Stem Compression in Chiari I Patients.”European Spine Journal, Springer-Verlag, Sept. 2008, <www.ncbi.nlm.nih.gov/pmc/articles/PMC2527411/>.
Disclaimer: The information provided on our website is strictly for educational purposes in order to help further the understanding of Chiari and its associated conditions. You should in no way use this site as a replacement for diagnosis, treatment, or medical advice from a qualified medical professional.








 One of the biggest hurdles a Chiari patient may face is that of simply being diagnosed. Some studies cite an average of 5 years between the onset of symptoms significant enough for a patient to seek medical care and the patient receiving an accurate diagnosis of Chiari Malformation. Sadly, however, online support groups and message boards are peppered with the stories of patients who went undiagnosed, or more often, misdiagnosed, for decades. Patients are frequently misdiagnosed with conditions such as
One of the biggest hurdles a Chiari patient may face is that of simply being diagnosed. Some studies cite an average of 5 years between the onset of symptoms significant enough for a patient to seek medical care and the patient receiving an accurate diagnosis of Chiari Malformation. Sadly, however, online support groups and message boards are peppered with the stories of patients who went undiagnosed, or more often, misdiagnosed, for decades. Patients are frequently misdiagnosed with conditions such as  Diagnosis of Chiari Malformation is based upon the presence of Chiari symptoms, such as an
Diagnosis of Chiari Malformation is based upon the presence of Chiari symptoms, such as an  becoming apparent that Chiari is not quite as rare as it was once thought to be. When a primary care physician is stumped by a patient’s complaints of headaches and neurological symptoms, it is only natural to refer that patient to a
becoming apparent that Chiari is not quite as rare as it was once thought to be. When a primary care physician is stumped by a patient’s complaints of headaches and neurological symptoms, it is only natural to refer that patient to a